Department of Public Health Sciences, University of Miami Miller School of Medicine, Miami, FL, USA.
RTI International, Research Triangle Park, NC, USA.
Addict Sci Clin Pract. 2024 Apr 2;19(1):23. doi: 10.1186/s13722-024-00454-w.
Communities That HEAL (CTH) is a novel, data-driven community-engaged intervention designed to reduce opioid overdose deaths by increasing community engagement, adoption of an integrated set of evidence-based practices, and delivering a communications campaign across healthcare, behavioral-health, criminal-legal, and other community-based settings. The implementation of such a complex initiative requires up-front investments of time and other expenditures (i.e., start-up costs). Despite the importance of these start-up costs in investment decisions to stakeholders, they are typically excluded from cost-effectiveness analyses. The objective of this study is to report a detailed analysis of CTH start-up costs pre-intervention implementation and to describe the relevance of these data for stakeholders to determine implementation feasibility.
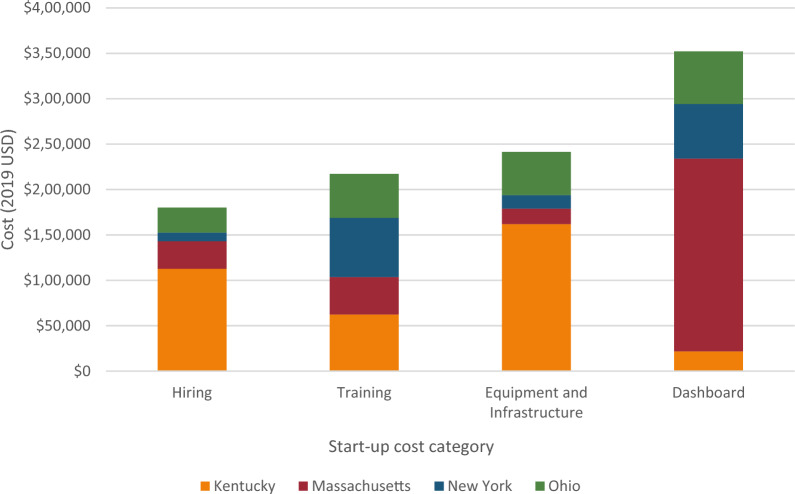
This study is guided by the community perspective, reflecting the investments that a real-world community would need to incur to implement the CTH intervention. We adopted an activity-based costing approach, in which resources related to hiring, training, purchasing, and community dashboard creation were identified through macro- and micro-costing techniques from 34 communities with high rates of fatal opioid overdoses, across four states-Kentucky, Massachusetts, New York, and Ohio. Resources were identified and assigned a unit cost using administrative and semi-structured-interview data. All cost estimates were reported in 2019 dollars.
State-level average and median start-up cost (representing 8-10 communities per state) were $268,657 and $175,683, respectively. Hiring and training represented 40%, equipment and infrastructure costs represented 24%, and dashboard creation represented 36% of the total average start-up cost. Comparatively, hiring and training represented 49%, purchasing costs represented 18%, and dashboard creation represented 34% of the total median start-up cost.
We identified three distinct CTH hiring models that affected start-up costs: hospital-academic (Massachusetts), university-academic (Kentucky and Ohio), and community-leveraged (New York). Hiring, training, and purchasing start-up costs were lowest in New York due to existing local infrastructure. Community-based implementation similar to the New York model may have lower start-up costs due to leveraging of existing infrastructure, relationships, and support from local health departments.
社区康复(CTH)是一种新颖的数据驱动的社区参与干预措施,旨在通过增加社区参与、采用一套综合的循证实践以及在医疗保健、行为健康、刑事法律和其他社区环境中开展宣传活动,来减少阿片类药物过量死亡。实施这样一个复杂的计划需要预先投入时间和其他支出(即启动成本)。尽管这些启动成本对于利益相关者的投资决策很重要,但它们通常被排除在成本效益分析之外。本研究的目的是报告 CTH 干预实施前的详细启动成本分析,并描述这些数据与利益相关者的相关性,以确定实施的可行性。
本研究以社区为视角,反映了现实社区实施 CTH 干预所需的投资。我们采用了基于活动的成本核算方法,通过来自四个州(肯塔基州、马萨诸塞州、纽约州和俄亥俄州)的 34 个致命阿片类药物过量率较高的社区的宏观和微观成本核算技术,确定了与招聘、培训、采购和社区仪表板创建相关的资源。使用行政和半结构化访谈数据确定资源并分配单位成本。所有成本估算均以 2019 年美元报告。
州一级的平均和中位数启动成本(每个州代表 8-10 个社区)分别为 268657 美元和 175683 美元。招聘和培训占 40%,设备和基础设施成本占 24%,仪表板创建占总平均启动成本的 36%。相比之下,招聘和培训占 49%,采购成本占 18%,仪表板创建占总中位数启动成本的 34%。
我们确定了三种不同的 CTH 招聘模式,这些模式影响了启动成本:医院-学术模式(马萨诸塞州)、大学-学术模式(肯塔基州和俄亥俄州)和社区杠杆模式(纽约州)。由于现有的地方基础设施,纽约州的招聘、培训和采购启动成本最低。由于利用现有基础设施、关系和当地卫生部门的支持,类似于纽约模式的社区实施可能会降低启动成本。