Galli Anaïs, Ma'ani Abuzahra Yaman, Bänziger Carola, Ballo Aboubacar, Friedrich Max N D, Gross Karin, Harter Miriam, Hattendorf Jan, Peter Maryna, Tamas Andrea, Owen Branwen N, Winkler Mirko S
Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, Allschwil, Switzerland.
Faculty of Natural Sciences, University of Basel, Basel, Switzerland.
JMIR Res Protoc. 2024 Apr 3;13:e52959. doi: 10.2196/52959.
Hand hygiene is crucial in health care centers and schools to avoid disease transmission. Currently, little is known about hand hygiene in such facilities in protracted conflict settings.
This protocol aims to assess the effectiveness of a multicomponent hand hygiene intervention on handwashing behavior, underlying behavioral factors, and the well-being of health care workers and students. Moreover, we report our methodology and statistical analysis plan transparently.
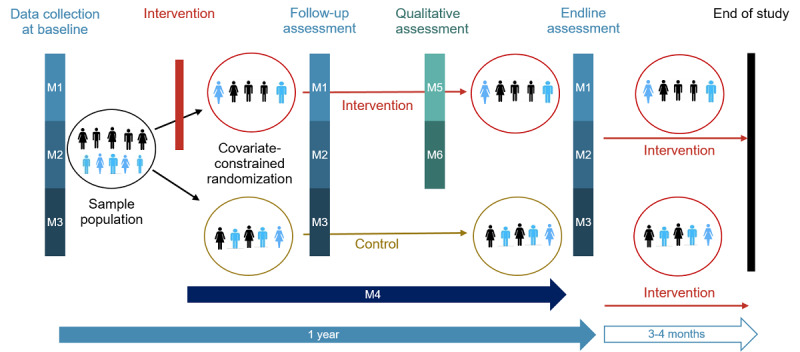
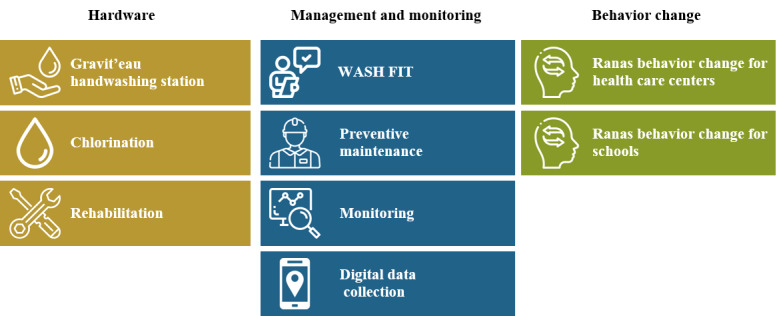
This is a cluster randomized controlled trial with 2 parallel arms taking place in 4 countries for 1 year. In Burkina Faso and Mali, we worked in 24 primary health care centers per country, whereas in Nigeria and Palestine, we focused on 26 primary schools per country. Facilities were eligible if they were not connected to a functioning water source but were deemed accessible to the implementation partners. Moreover, health care centers were eligible if they had a maternity ward and ≥5 employees, and schools if they had ≤7000 students studying in grades 5 to 7. We used covariate-constrained randomization to assign intervention facilities that received a hardware, management and monitoring support, and behavior change. Control facilities will receive the same or improved intervention after endline data collection. To evaluate the intervention, at baseline and endline, we used a self-reported survey, structured handwashing observations, and hand-rinse samples. At follow-up, hand-rinse samples were dropped. Starting from the intervention implementation, we collected longitudinal data on hygiene-related health conditions and absenteeism. We also collected qualitative data with focus group discussions and interviews. Data were analyzed descriptively and with random effect regression models with the random effect at a cluster level. The primary outcome for health centers is the handwashing rate, defined as the number of times health care workers performed good handwashing practice with soap or alcohol-based handrub at one of the World Health Organization 5 moments for hand hygiene, divided by the number of moments for hand hygiene that presented themselves during the patient interaction within an hour of observation. For schools, the primary outcome is the number of students who washed their hands before eating.
The baseline data collection across all countries lasted from February to June 2023. We collected data from 135 and 174 health care workers in Burkina Faso and Mali, respectively. In Nigeria, we collected data from 1300 students and in Palestine from 1127 students. The endline data collection began in February 2024.
This is one of the first studies investigating hand hygiene in primary health care centers and schools in protracted conflict settings. With our strong study design, we expect to support local policy makers and humanitarian organizations in developing sustainable agendas for hygiene promotion.
ClinicalTrials.gov NCT05946980 (Burkina Faso and Mali); https://www.clinicaltrials.gov/study/NCT05946980 and NCT05964478 (Nigeria and Palestine); https://www.clinicaltrials.gov/study/NCT05964478.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/52959.
在医疗保健中心和学校,手部卫生对于避免疾病传播至关重要。目前,对于长期冲突地区此类场所的手部卫生情况知之甚少。
本方案旨在评估多组分手部卫生干预措施对洗手行为、潜在行为因素以及医护人员和学生健康状况的有效性。此外,我们将透明地报告我们的方法和统计分析计划。
这是一项整群随机对照试验,在4个国家进行,为期1年,有2个平行组。在布基纳法索和马里,我们在每个国家的24个初级卫生保健中心开展工作,而在尼日利亚和巴勒斯坦,我们专注于每个国家的26所小学。如果设施未连接到正常运行的水源,但实施伙伴认为可以到达,则符合条件。此外,初级卫生保健中心若设有产科病房且有≥5名员工,学校若有≤7000名五至七年级的学生,则符合条件。我们采用协变量约束随机化方法来分配接受硬件、管理与监测支持以及行为改变的干预设施。对照设施将在终末数据收集后接受相同或改进的干预措施。为了评估干预效果,在基线和终末时,我们使用了自我报告调查、结构化洗手观察和洗手样本。在随访时,不再采集洗手样本。从干预措施实施开始,我们收集了与卫生相关的健康状况和缺勤情况的纵向数据。我们还通过焦点小组讨论和访谈收集了定性数据。数据采用描述性分析,并使用整群水平具有随机效应的随机效应回归模型进行分析。卫生中心的主要结局是洗手率,定义为医护人员在世界卫生组织的5个手部卫生关键时刻之一,使用肥皂或酒精类洗手液进行良好洗手的次数,除以观察一小时内与患者互动期间出现的手部卫生关键时刻的次数。对于学校,主要结局是饭前洗手的学生人数。
所有国家的基线数据收集从2023年2月持续到6月。我们分别从布基纳法索的135名和马里的174名医护人员那里收集了数据。在尼日利亚,我们收集了1300名学生的数据,在巴勒斯坦收集了1127名学生的数据。终末数据收集于2024年2月开始。
这是首批调查长期冲突地区初级卫生保健中心和学校手部卫生情况的研究之一。凭借我们强大的研究设计,我们期望支持当地政策制定者和人道主义组织制定可持续的卫生促进议程。
ClinicalTrials.gov NCT05946980(布基纳法索和马里);https://www.clinicaltrials.gov/study/NCT05946980 以及 NCT05964478(尼日利亚和巴勒斯坦);https://www.clinicaltrials.gov/study/NCT05964478。
国际注册报告识别码(IRRID):DERR1-10.2196/52959。