Department of Obstetrics and Gynecology, The Jikei University School of Medicine, Tokyo, Japan.
Department of Gynecology, National Center Cancer Hospital East, Kashiwa, Japan.
J Gynecol Oncol. 2024 Nov;35(6):e76. doi: 10.3802/jgo.2024.35.e76. Epub 2024 Mar 26.
This study compared the effectiveness, safety, and tolerability of dose-dense paclitaxel and carboplatin plus bevacizumab (ddTC+Bev) with ddTC for advanced ovarian cancer.
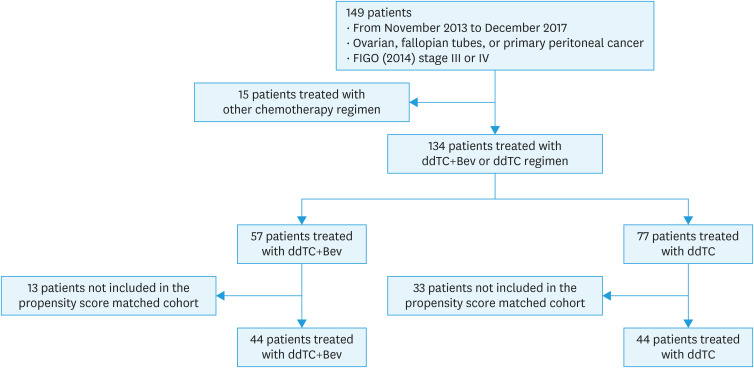
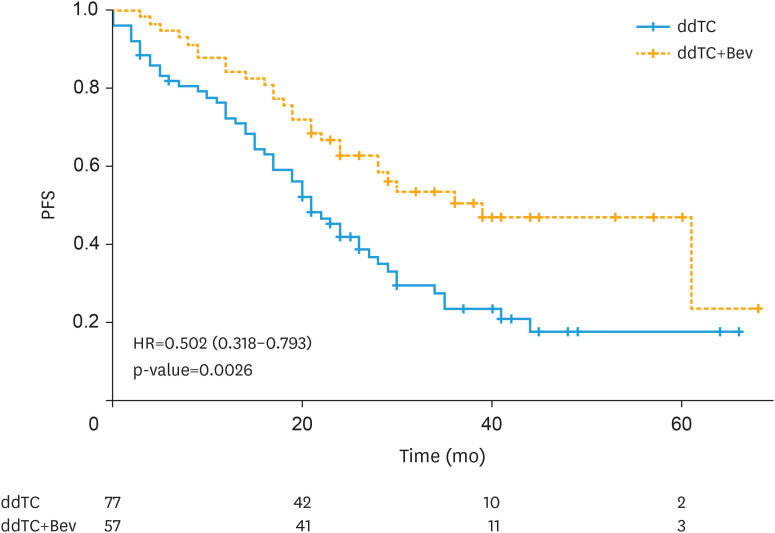
We retrospectively analyzed the clinical records of 134 patients who received ddTC+Bev or ddTC as first-line chemotherapy for stage III-IV ovarian cancer. Progression-free survival as primary endpoint of this study was compared using the log-rank test. Cox proportional hazards model and propensity score matching (PSM) were used to analyze prognostic factors, and the frequency of adverse events was examined using the χ² test.
We categorized 134 patients in the ddTC+Bev (n=57) and ddTC (n=77) groups who started treatment at four related institutions from November 2013 to December 2017. No patients used poly (ADP-ribose) polymerase inhibitors as the first line maintenance therapy. The progression-free survival (PFS) of the ddTC+Bev group had a significantly better prognosis than that of the ddTC group (hazard ratio [HR]=0.50; 95% confidence interval [CI]=0.32-0.79; p<0.003). Multivariate analysis showed that ddTC+Bev regimen was a prognostic factor. However, intergroup comparison using PSM revealed that the PFS of the ddTC+Bev group had a nonsignificantly better prognosis than that of the ddTC group (HR=0.70; 95% CI=0.41-1.20; p=0.189). Few adverse events above G3 were noted for ddTC+Bev, which were sufficiently tolerable.
This study could not demonstrate that adding Bev to ddTC improves prognosis. Further studies with more cases are warranted.
本研究比较了剂量密集型紫杉醇和卡铂联合贝伐珠单抗(ddTC+Bev)与 ddTC 治疗晚期卵巢癌的疗效、安全性和耐受性。
我们回顾性分析了 134 例接受 ddTC+Bev 或 ddTC 作为一线化疗治疗 III-IV 期卵巢癌的患者的临床记录。采用对数秩检验比较无进展生存期作为主要研究终点。采用 Cox 比例风险模型和倾向评分匹配(PSM)分析预后因素,采用卡方检验分析不良事件发生频率。
我们将 2013 年 11 月至 2017 年 12 月在四家相关机构接受治疗的 134 例患者分为 ddTC+Bev(n=57)和 ddTC(n=77)组。没有患者使用聚(ADP-核糖)聚合酶抑制剂作为一线维持治疗。ddTC+Bev 组的无进展生存期(PFS)预后明显优于 ddTC 组(风险比[HR]=0.50;95%置信区间[CI]=0.32-0.79;p<0.003)。多因素分析显示,ddTC+Bev 方案是一个预后因素。然而,采用 PSM 进行的组间比较显示,ddTC+Bev 组的 PFS 预后无显著改善(HR=0.70;95%CI=0.41-1.20;p=0.189)。ddTC+Bev 组的不良反应大多为 G3 级以下,可耐受。
本研究未能证明在 ddTC 中加入 Bev 可改善预后。需要更多病例的进一步研究。