Arumugam Sankar, Sidhom Mark
Department of Medical Physics, Liverpool and Macarthur Cancer Therapy Centres and Ingham Institute, New South Wales, Australia.
South Western Sydney, Clinical School, University of New South Wales, Sydney, New South Wales, Australia.
Adv Radiat Oncol. 2024 Feb 6;9(5):101455. doi: 10.1016/j.adro.2024.101455. eCollection 2024 May.
To assess the robustness of the dose delivered to the clinical target volume (CTV) between planning target volume (PTV)-based and robust optimization planning approaches in localized prostate cancer radiation therapy.
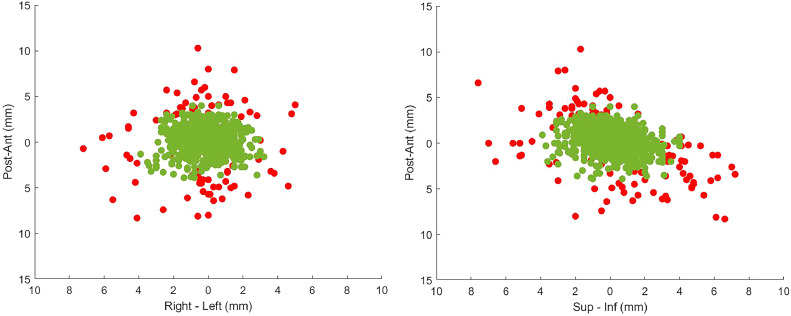
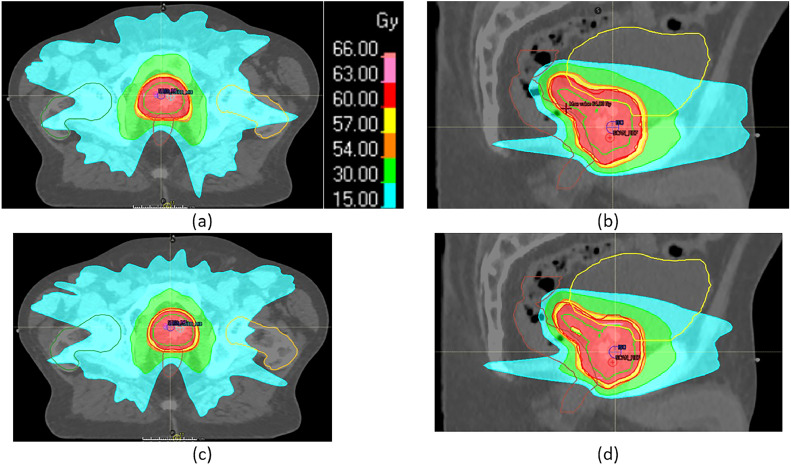
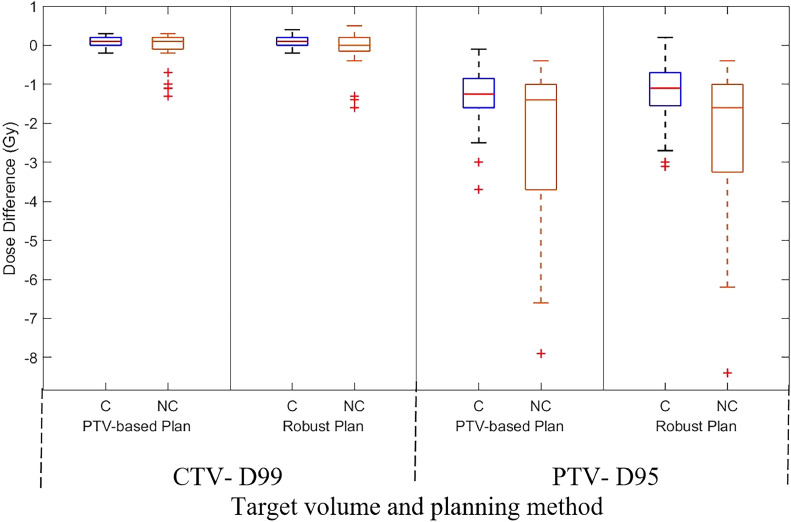
Retrospective data of 20 patients with prostate cancer, including radiation therapy and real-time prostate position, were analyzed. Two sets of volumetric modulated arc therapy plans were generated per patient: PTV-based and robust optimization. PTV-based planning used a 7-mm CTV-PTV margin, whereas robust planning considered same-magnitude position deviations. Differences in CTV dose delivered to 99% volume (D99), PTV dose delivered to 95% volume (D95), and bladder and rectum V40 (volume receiving 40 Gy) and V60 (volume receiving 60 Gy) values were evaluated. The target position, determined by in-house position monitoring system, was incorporated for dose assessment with and without position deviation correction.
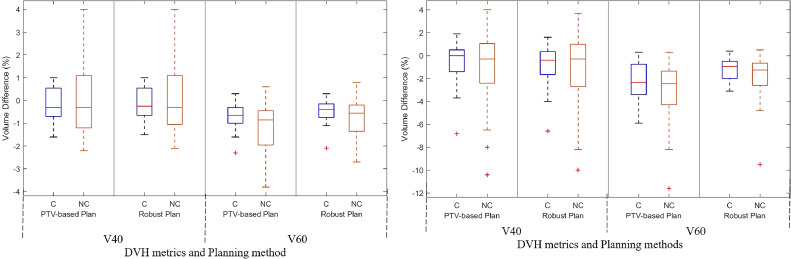
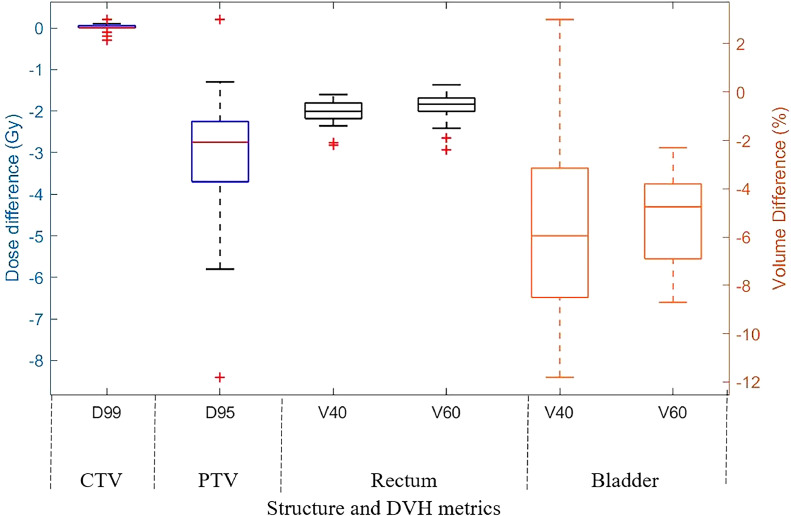
In the robust optimization approach, compared with PTV-based planning, the mean (standard deviation) V40 and V60 values of the bladder were reduced by 5.2% (4.1%) and 5.1% (1.9%), respectively. Similarly, for the rectum, the reductions were 0.8% (0.5%) and 0.6% (0.6%). In corrected treatment scenarios, both planning approaches resulted in a mean (standard deviation) CTV D99 difference of 0.1 Gy (0.1 Gy). In the not corrected scenario, PTV-based planning reduced CTV D99 by 0.1 Gy (0.5 Gy), whereas robust planning reduced it by 0.2 Gy (0.6 Gy). There was no statistically significant difference observed in the planned and delivered rectum and bladder dose for both corrected and not corrected scenarios.
Robust optimization resulted in lower V40 and V60 values for the bladder compared with PTV-based planning. However, no difference in CTV dose accuracy was found between the 2 approaches.
评估在局限性前列腺癌放射治疗中,基于计划靶体积(PTV)的计划和稳健优化计划方法之间,临床靶体积(CTV)所接受剂量的稳健性。
分析了20例前列腺癌患者的回顾性数据,包括放射治疗和前列腺实时位置。为每位患者生成了两组容积调强弧形治疗计划:基于PTV的计划和稳健优化计划。基于PTV的计划使用7毫米的CTV-PTV边界,而稳健计划考虑相同幅度的位置偏差。评估了CTV接受99%体积的剂量(D99)、PTV接受95%体积的剂量(D95)以及膀胱和直肠的V40(接受40 Gy的体积)和V60(接受60 Gy的体积)值的差异。通过内部位置监测系统确定的靶位置,用于有和没有位置偏差校正的剂量评估。
在稳健优化方法中,与基于PTV的计划相比,膀胱的平均(标准差)V40和V60值分别降低了5.2%(4.1%)和5.1%(1.9%)。同样,直肠的降低幅度分别为0.8%(0.5%)和0.6%(0.6%)。在校正后的治疗方案中,两种计划方法导致的CTV D99平均(标准差)差异为0.1 Gy(0.1 Gy)。在未校正的方案中,基于PTV的计划使CTV D99降低了0.1 Gy(0.5 Gy),而稳健计划使其降低了0.2 Gy(0.6 Gy)。在校正和未校正的方案中,计划和实际给予的直肠和膀胱剂量均未观察到统计学上的显著差异。
与基于PTV的计划相比,稳健优化使膀胱的V40和V60值更低。然而,两种方法在CTV剂量准确性方面未发现差异。