Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
Institute for Breast Cancer Precision Medicine, Yonsei University College of Medicine, Seoul, Republic of Korea.
Breast Cancer Res. 2024 Apr 12;26(1):65. doi: 10.1186/s13058-024-01816-7.
Sentinel lymph node biopsy (SLNB) is recommended for patients with ductal carcinoma in situ (DCIS) undergoing mastectomy, given the concerns regarding upstaging and technical difficulties of post-mastectomy SLNB. However, this may lead to potential overtreatment, considering favorable prognosis and de-escalation trends in DCIS. Data regarding upstaging and axillary lymph node metastasis among these patients remain limited.
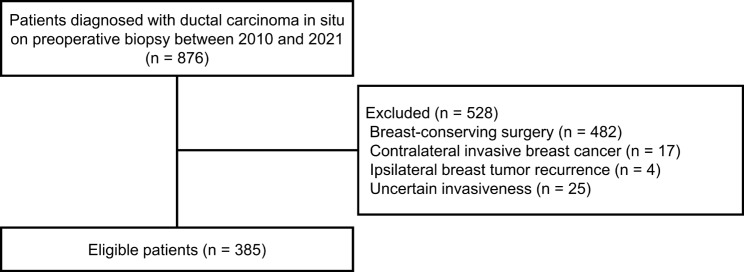
We retrospectively reviewed patients with DCIS who underwent mastectomy with SLNB or axillary lymph node dissection at Gangnam Severance Hospital between January 2010 and December 2021. To explore the feasibility of omitting SLNB, we assessed the rates of DCIS upgraded to invasive carcinoma and axillary lymph node metastasis. Binary Cox regression analysis was performed to identify clinicopathologic factors associated with upstaging and axillary lymph node metastasis.
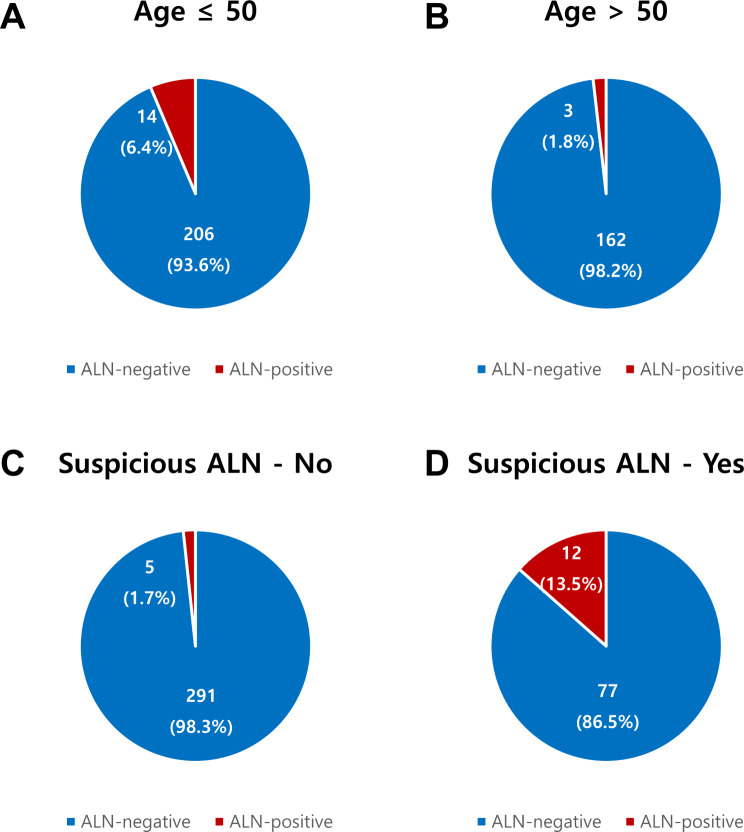
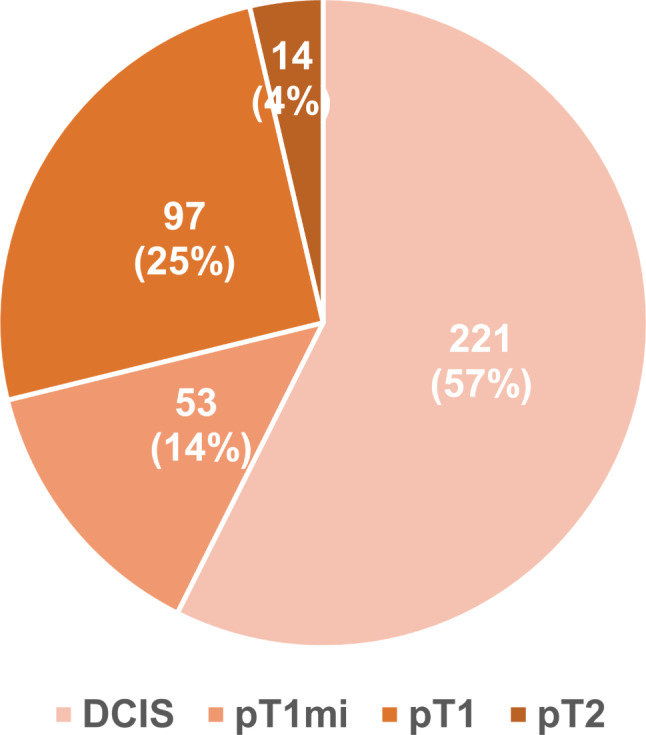
Among 385 patients, 164 (42.6%) experienced an invasive carcinoma upgrade: microinvasion, pT1, and pT2 were confirmed in 53 (13.8%), 97 (25.2%), and 14 (3.6%) patients, respectively. Seventeen (4.4%) patients had axillary lymph node metastasis. Multivariable analysis identified age ≤ 50 years (adjusted odds ratio [OR], 12.73; 95% confidence interval [CI], 1.18-137.51; p = 0.036) and suspicious axillary lymph nodes on radiologic evaluation (adjusted OR, 9.31; 95% CI, 2.06-41.99; p = 0.004) as independent factors associated with axillary lymph node metastasis. Among patients aged > 50 years and/or no suspicious axillary lymph nodes, only 1.7-2.3%) experienced axillary lymph node metastasis.
Although underestimation of the invasive component was relatively high among patients with DCIS undergoing mastectomy, axillary lymph node metastasis was rare. Our findings suggest that omitting SLNB may be feasible for patients over 50 and/or without suspicious axillary lymph nodes on radiologic evaluation.
鉴于导管原位癌(DCIS)患者行乳房切除术时存在升级分期和乳房切除术后前哨淋巴结活检(SLNB)技术难度的问题,建议对其行 SLNB。然而,考虑到 DCIS 的良好预后和降级趋势,这可能导致过度治疗。关于这些患者的升级分期和腋窝淋巴结转移的数据仍然有限。
我们回顾性分析了 2010 年 1 月至 2021 年 12 月在江南塞弗伦斯医院行乳房切除术并同时接受 SLNB 或腋窝淋巴结清扫术的 DCIS 患者。为了探讨省略 SLNB 的可行性,我们评估了 DCIS 升级为浸润性癌和腋窝淋巴结转移的发生率。采用二项 Cox 回归分析确定与升级分期和腋窝淋巴结转移相关的临床病理因素。
在 385 例患者中,有 164 例(42.6%)发生浸润性癌升级:微浸润、pT1 和 pT2 分别在 53 例(13.8%)、97 例(25.2%)和 14 例(3.6%)患者中确诊。17 例(4.4%)患者发生腋窝淋巴结转移。多变量分析显示,年龄≤50 岁(调整优势比[OR],12.73;95%置信区间[CI],1.18-137.51;p=0.036)和影像学评估可疑腋窝淋巴结(调整 OR,9.31;95%CI,2.06-41.99;p=0.004)是与腋窝淋巴结转移相关的独立因素。在年龄>50 岁和/或无可疑腋窝淋巴结的患者中,仅 1.7-2.3%发生腋窝淋巴结转移。
尽管行乳房切除术的 DCIS 患者中浸润性成分的低估相对较高,但腋窝淋巴结转移罕见。我们的研究结果表明,对于年龄>50 岁和/或影像学评估无可疑腋窝淋巴结的患者,省略 SLNB 可能是可行的。