Department of Digestive Tract and General Surgery, Saitama Medical Center, Saitama Medical University, 1981 Kamoda, Kawagoe, Saitama, 350-8550, Japan.
Department of Surgery, Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital, Tokyo, Japan.
Int J Clin Oncol. 2024 Jul;29(7):953-963. doi: 10.1007/s10147-024-02518-y. Epub 2024 Apr 14.
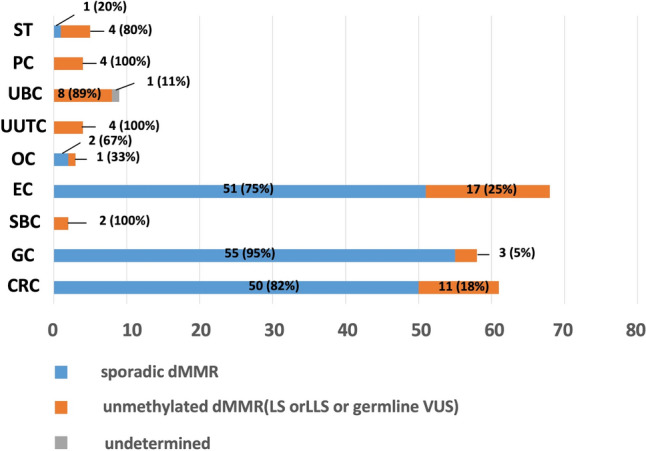
Based on molecular characteristics, deficient DNA mismatch repair (dMMR) solid tumors are largely divided into three categories: somatically MLH1-hypermethylated tumors, Lynch syndrome (LS)-associated tumors, and Lynch-like syndrome (LLS)-associated tumors. The incidence of each of these conditions and the corresponding pathogenic genes related to LLS remain elusive.
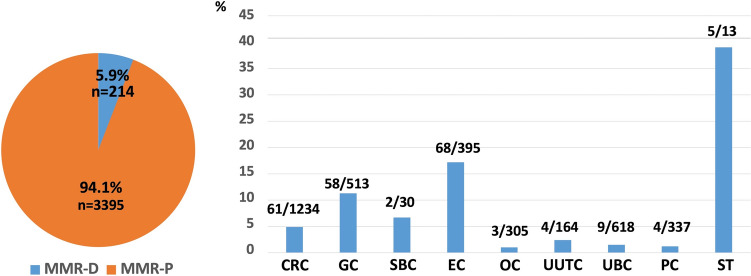
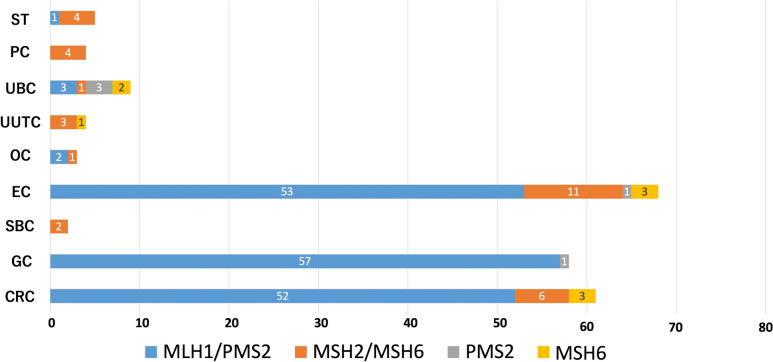
We identified dMMR tumors in 3609 tumors from 9 different solid organs, including colorectal cancer, gastric cancer, small-bowel cancer, endometrial cancer, ovarian cancer, upper urinary tract cancer, urinary bladder cancer, prostate cancer, and sebaceous tumor, and comprehensively summarized the characterization of dMMR tumors. Characterization of dMMR tumors were performed as loss of at least one of MMR proteins (MLH1, MSH2, MSH6, and PMS2), by immunohistochemistry, followed by MLH1 promotor methylation analysis and genetic testing for MMR genes where appropriate. Somatic variant analysis of MMR genes and whole exome sequencing (WES) were performed in patients with LLS.
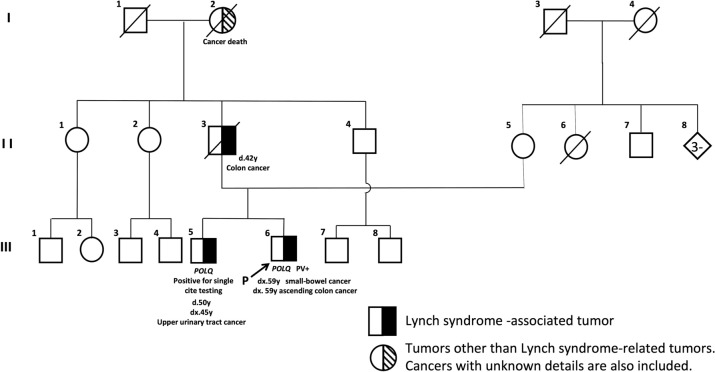
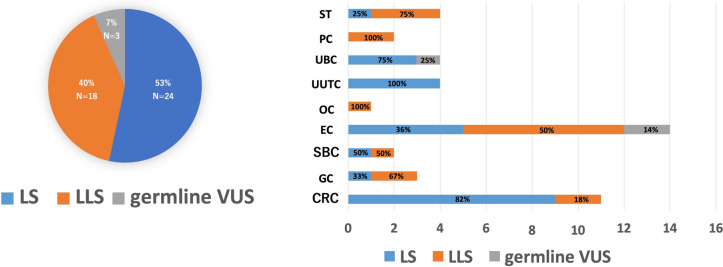
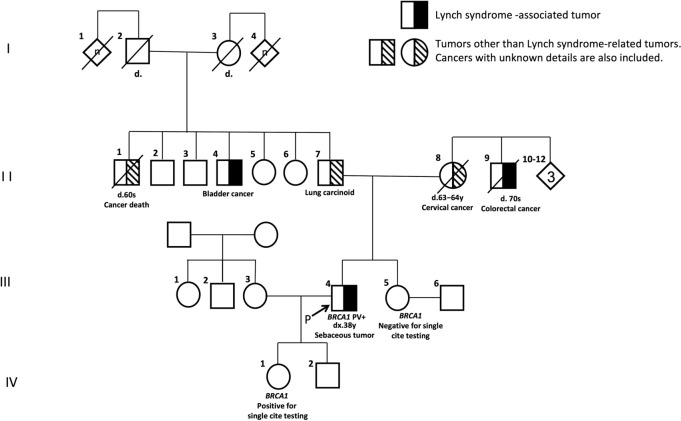
In total, the incidence of dMMR tumors was 5.9% (24/3609). The incidence of dMMR tumors and the proportion of the three categorized dMMR tumors varied considerably with different tumor types. One to three likely pathogenic/pathogenic somatic MMR gene variants were detected in 15 out of the 16 available LLS tumors. One patient each from 12 patients who gave consent to WES demonstrated non-MMR germline variants affect function (POLQ or BRCA1).
Our data regarding the LS to LLS ratio would be useful for genetic counseling in patients who are suspected to have LS, though the genetic backgrounds for the pathogenesis of LLS need further investigation.
基于分子特征,存在缺陷的 DNA 错配修复(dMMR)实体瘤主要分为三类:体细胞 MLH1 高甲基化肿瘤、林奇综合征(LS)相关肿瘤和林奇样综合征(LLS)相关肿瘤。这些情况中的每一种的发生率以及与 LLS 相关的相应致病基因仍不明确。
我们在 9 种不同实体器官的 3609 个肿瘤中鉴定出 dMMR 肿瘤,包括结直肠癌、胃癌、小肠癌、子宫内膜癌、卵巢癌、上尿路上皮癌、膀胱癌、前列腺癌和皮脂腺瘤,并全面总结了 dMMR 肿瘤的特征。通过免疫组织化学分析,dMMR 肿瘤的特征表现为至少一种 MMR 蛋白(MLH1、MSH2、MSH6 和 PMS2)的缺失,随后进行 MLH1 启动子甲基化分析,并在适当情况下对 MMR 基因进行遗传检测。对 LLS 患者的 MMR 基因进行体细胞变异分析和全外显子组测序(WES)。
总共,dMMR 肿瘤的发生率为 5.9%(24/3609)。不同肿瘤类型的 dMMR 肿瘤发生率和三种分类的 dMMR 肿瘤的比例差异很大。在 16 例可获得的 LLS 肿瘤中有 15 例检测到 1 到 3 个可能的致病性/致病性体细胞 MMR 基因变异。在同意进行 WES 的 12 名患者中,各有 1 名患者存在影响功能的非 MMR 种系变异(POLQ 或 BRCA1)。
我们关于 LS 与 LLS 比例的数据对于疑似 LS 的患者的遗传咨询将很有用,尽管 LLS 发病机制的遗传背景仍需要进一步研究。