Division of Evolution and Genomic Medicine, The University of Manchester, Manchester, UK.
Clinical Genetics Service, Manchester Centre for Genomic Medicine, North-West Genomics Laboratory Hub, Manchester University NHS Foundation Trust, Manchester, Greater Manchester, UK.
J Med Genet. 2022 Apr;59(4):328-334. doi: 10.1136/jmedgenet-2020-107542. Epub 2021 Jan 15.
Testing cancers for mismatch repair deficiency (dMMR) by immunohistochemistry (IHC) is a quick and inexpensive means of triaging individuals for germline Lynch syndrome testing. The aim of this study was to evaluate tumour dMMR and the prevalence of Lynch syndrome in patients referred to the Manchester Centre for Genomic Medicine, which serves a population of 5.6 million.
Tumour testing used IHC for MMR proteins with targeted and promotor methylation testing followed by germline mutation and somatic testing as appropriate.
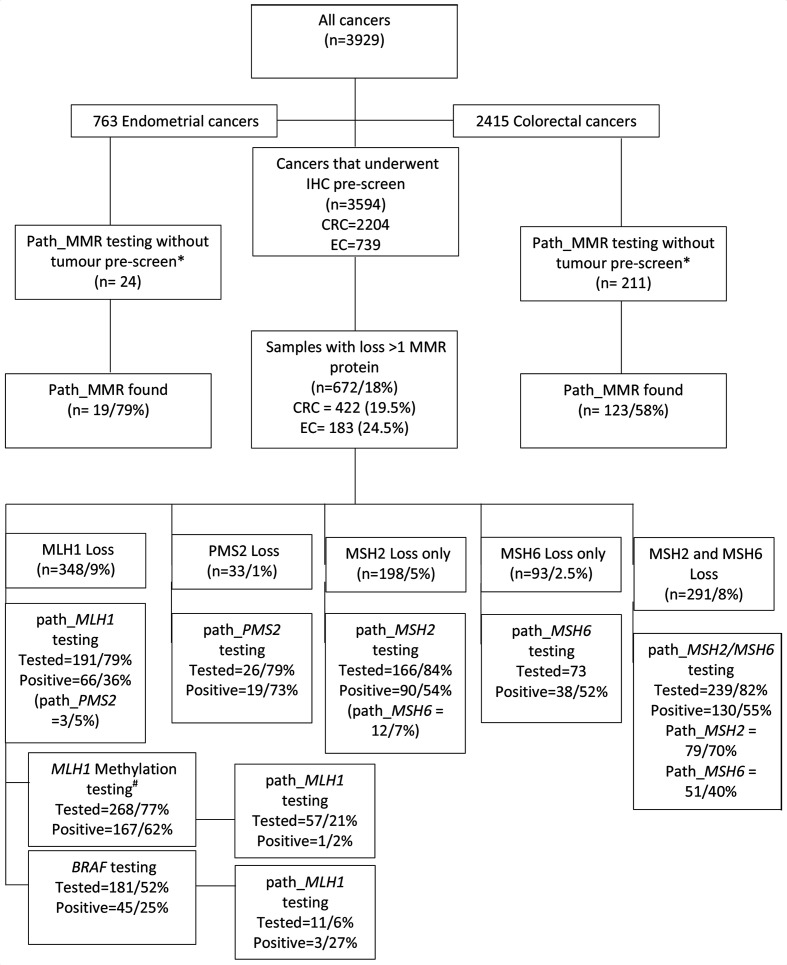
In total, 3694 index tumours were tested by IHC (2204 colorectal cancers (CRCs), 739 endometrial cancers (ECs) and 761 other), of which 672/3694 (18.2%) had protein loss, including 348 (9.4%) with MLH1 loss. MLH1 loss was significantly higher for 739 ECs (15%) vs 2204 CRCs (10%) (p=0.0003) and was explained entirely by higher rates of somatic promoter hypermethylation (87% vs 41%, p<0.0001). Overall, 65/134 (48.5%) patients with MLH1 loss and no hypermethylation or c.1799T>A had constitutional pathogenic variants. Of 456 patients with tumours showing loss of MSH2/MSH6, 216 (47.3%) had germline pathogenic variants in either gene. Isolated PMS2 loss was most suggestive of a germline MMR variant in 19/26 (73%). Of those with no germline pathogenic variant, somatic testing identified likely causal variants in 34/48 (71%) with MLH1 loss and in in 40/47 (85%) with MSH2/MSH6 loss.
Reflex testing of EC/CRC leads to uncertain diagnoses in many individuals with dMMR following IHC but without germline pathogenic variants or hypermethylation. Tumour mutation testing is effective at decreasing this by identifying somatic dMMR in >75% of cases.
通过免疫组织化学(IHC)检测错配修复缺陷(dMMR)是一种快速且廉价的方法,可以对林奇综合征种系检测进行初步筛选。本研究旨在评估曼彻斯特基因组医学中心就诊患者的肿瘤 dMMR 发生率和林奇综合征的患病率,该中心服务于 560 万人口。
肿瘤检测采用 MMR 蛋白的 IHC,同时进行 和 启动子甲基化靶向检测,然后根据需要进行种系突变和体细胞检测。
总共对 3694 个索引肿瘤进行了 IHC 检测(2204 例结直肠癌(CRC)、739 例子宫内膜癌(EC)和 761 例其他肿瘤),其中 672/3694(18.2%)存在蛋白丢失,包括 348(9.4%)例 MLH1 丢失。739 例 EC 中 MLH1 丢失率明显高于 2204 例 CRC(15% vs. 10%)(p=0.0003),这完全由更高的体细胞 启动子高甲基化率(87% vs. 41%)引起(p<0.0001)。总体而言,134 例 MLH1 丢失且无 高甲基化或 c.1799T>A 的患者中,有 65/134(48.5%)例存在种系 致病性变异。在 456 例表现为 MSH2/MSH6 丢失的患者中,有 216(47.3%)例在任一基因中存在种系致病性变异。单独的 PMS2 丢失在 26 例(73%)中最提示存在种系 MMR 变异,在无种系致病性变异的患者中,MLH1 丢失患者中有 34/48(71%)例和 MSH2/MSH6 丢失患者中有 40/47(85%)例通过体细胞检测发现了可能的因果变异。
IHC 检测后,EC/CRC 患者出现 dMMR 时,进行反射性检测会导致许多患者出现不确定的诊断,但没有种系致病性变异或 高甲基化。肿瘤突变检测可有效减少这种情况,超过 75%的病例可通过识别体细胞 dMMR 来确定。