Department of Anaesthesia & Intensive Care, Cerrahpasa Medical Faculty, Istanbul University-Cerrahpasa, University of Istanbul, 34098, Cerrahpasa, Istanbul, Turkey.
Acta Neurochir (Wien). 2024 Apr 15;166(1):177. doi: 10.1007/s00701-024-06067-1.
In general, high levels of PEEP application is avoided in patients undergoing craniotomy to prevent a rise in ICP. But that approach would increase the risk of secondary brain injury especially in hypoxemic patients. Because the optic nerve sheath is distensible, a rise in ICP is associated with an increase in the optic nerve sheath diameter (ONSD). The cutoff value for elevated ICP assessed by ONSD is between 5.6 and 6.3 mm. We aimed to evaluate the effect of different PEEP levels on ONSD and compare the effect of different PEEP levels in patients with and without intracranial midline shift.
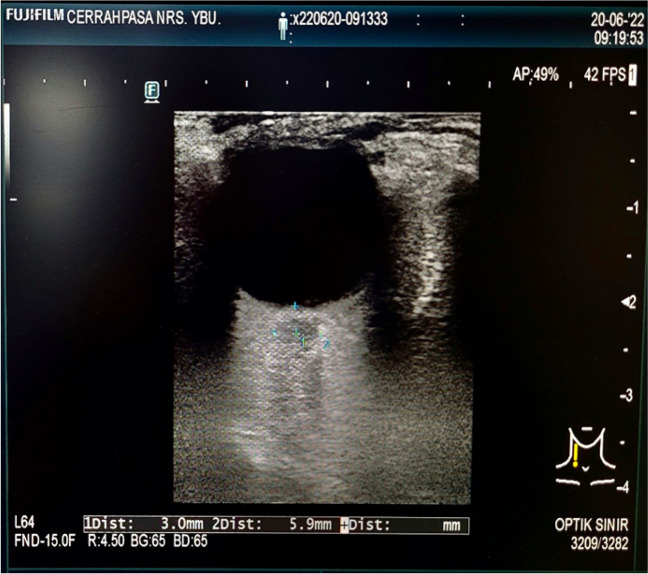
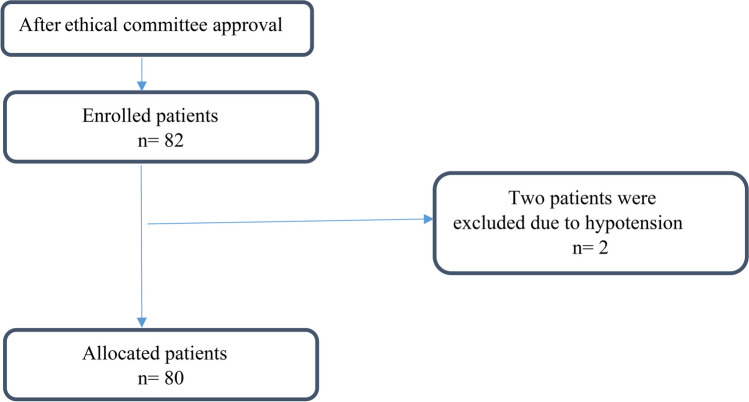
This prospective observational study was performed in aged 18-70 years, ASA I-III, 80 patients who were undergoing supratentorial craniotomy. After the induction of general anesthesia, the ONSD's were measured by the linear transducer from 3 mm below the globe at PEEP values of 0-5-10 cmHO. The ONSD were compered between patients with (n = 7) and without midline shift (n = 73) at different PEEP values.
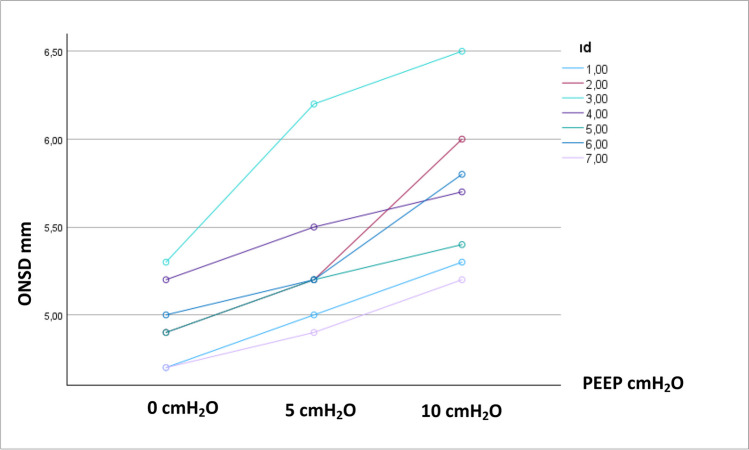
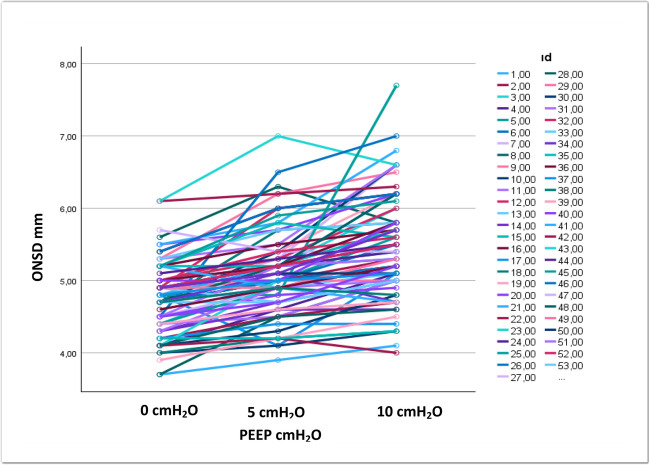
The increases in ONSD due to increase in PEEP level were determined (p < 0.001). No difference was found in the comparison of ONSD between patients with and without midline shift in different PEEP values (p = 0.329, 0.535, 0.410 respectively). But application of 10 cmHO PEEP in patients with a midline shift increased the mean ONSD value to 5.73 mm. This value is roughly 0.1 mm higher than the lower limit of the ONSD cutoff value.
The ONSD in adults undergoing supratentorial tumor craniotomy, PEEP values up to 5 cmHO, appears not to be associated with an ICP increase; however, the ONSD exceeded the cutoff for increased ICP when a PEEP of 10 cmHO was applied in patients with midline shift.
一般来说,为了防止颅内压升高,在接受开颅手术的患者中避免应用高水平的 PEEP。但这种方法会增加二次脑损伤的风险,尤其是在低氧血症患者中。由于视神经鞘具有可扩展性,颅内压升高与视神经鞘直径(ONSD)的增加相关。通过 ONSD 评估升高的 ICP 的截止值在 5.6 至 6.3 毫米之间。我们旨在评估不同 PEEP 水平对 ONSD 的影响,并比较颅内中线移位患者和无颅内中线移位患者的不同 PEEP 水平的影响。
这是一项前瞻性观察性研究,纳入了 80 名年龄在 18-70 岁、ASA I-III 级、接受幕上开颅手术的患者。在全身麻醉诱导后,通过线性换能器从眼球下方 3 毫米处测量 ONSD,在 PEEP 值为 0-5-10 cmHO 时进行测量。在不同的 PEEP 值下,比较有中线移位(n=7)和无中线移位(n=73)患者的 ONSD。
确定了由于 PEEP 水平增加导致的 ONSD 增加(p<0.001)。在不同 PEEP 值下,比较有中线移位和无中线移位患者的 ONSD 时,无差异(p=0.329、0.535、0.410 分别)。但在中线移位患者中应用 10 cmHO PEEP 会将平均 ONSD 值增加到 5.73 毫米。这个值比 ONSD 截止值的下限高约 0.1 毫米。
在接受幕上肿瘤开颅手术的成年人中,PEEP 值高达 5 cmHO 似乎与 ICP 升高无关;然而,当在中线移位患者中应用 10 cmHO PEEP 时,ONSD 超过了升高的 ICP 的截止值。