General Surgery Unit, Sandro Pertini Hospital, ASL Roma 2, Rome, Italy.
General Surgery Unit, Università degli Studi dell'Aquila, Via Vetoio, snc, 67100, L'Aquila, Italy.
Int J Colorectal Dis. 2024 Apr 16;39(1):53. doi: 10.1007/s00384-024-04627-6.
Current evidence concerning bowel preparation before elective colorectal surgery is still controversial. This study aimed to compare the incidence of anastomotic leakage (AL), surgical site infections (SSIs), and overall morbidity (any adverse event, OM) after elective colorectal surgery using four different types of bowel preparation.
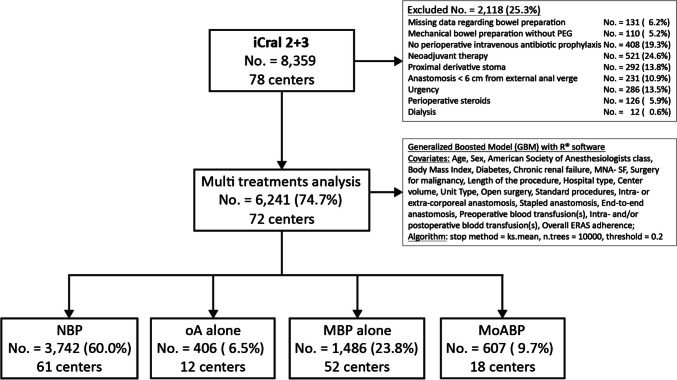
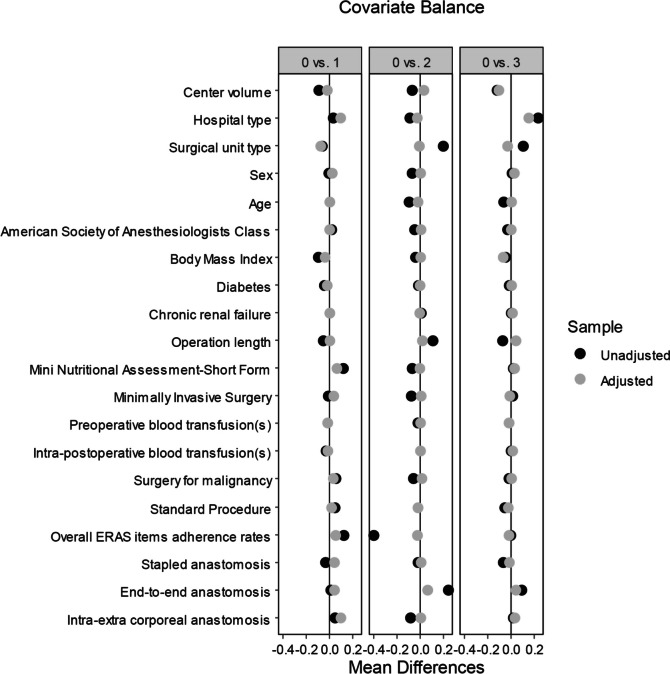
A prospective database gathered among 78 Italian surgical centers in two prospective studies, including 6241 patients who underwent elective colorectal resection with anastomosis for malignant or benign disease, was re-analyzed through a multi-treatment machine-learning model considering no bowel preparation (NBP; No. = 3742; 60.0%) as the reference treatment arm, compared to oral antibiotics alone (oA; No. = 406; 6.5%), mechanical bowel preparation alone (MBP; No. = 1486; 23.8%), or in combination with oAB (MoABP; No. = 607; 9.7%). Twenty covariates related to biometric data, surgical procedures, perioperative management, and hospital/center data potentially affecting outcomes were included and balanced into the model. The primary endpoints were AL, SSIs, and OM. All the results were reported as odds ratio (OR) with 95% confidence intervals (95% CI).
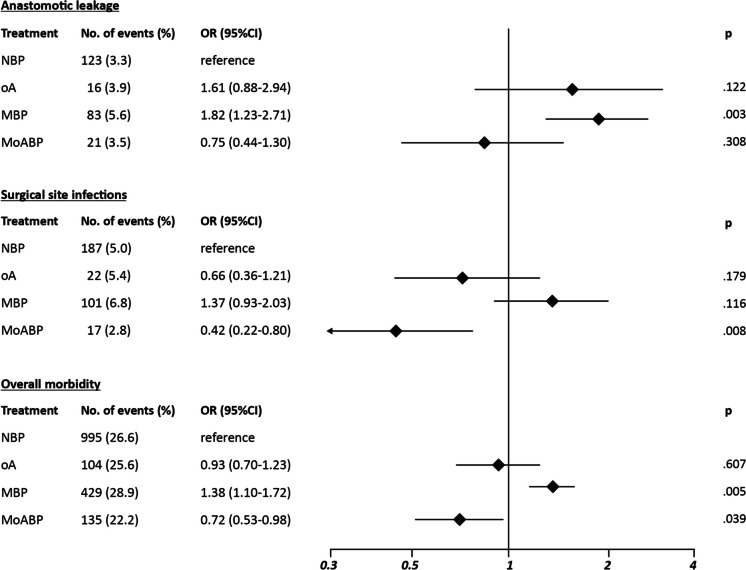
Compared to NBP, MBP showed significantly higher AL risk (OR 1.82; 95% CI 1.23-2.71; p = .003) and OM risk (OR 1.38; 95% CI 1.10-1.72; p = .005), no significant differences for all the endpoints were recorded in the oA group, whereas MoABP showed a significantly reduced SSI risk (OR 0.45; 95% CI 0.25-0.79; p = .008).
MoABP significantly reduced the SSI risk after elective colorectal surgery, therefore representing a valid alternative to NBP.
目前关于择期结直肠手术前肠道准备的证据仍存在争议。本研究旨在比较四种不同类型的肠道准备后择期结直肠手术吻合口漏(AL)、手术部位感染(SSI)和总体发病率(任何不良事件,OM)的发生率。
通过多治疗机器学习模型对 78 家意大利外科中心的两项前瞻性研究中的前瞻性数据库进行了重新分析,该模型考虑了无肠道准备(NBP;No. = 3742;60.0%)作为参考治疗组,与单独口服抗生素(oA;No. = 406;6.5%)、单独机械肠道准备(MBP;No. = 1486;23.8%)或与 oAB 联合(MoABP;No. = 607;9.7%)进行比较。纳入了 20 个与生物统计学数据、手术程序、围手术期管理和医院/中心数据相关的协变量,这些数据可能影响结果,并在模型中进行了平衡。主要终点是 AL、SSI 和 OM。所有结果均以比值比(OR)和 95%置信区间(95%CI)表示。
与 NBP 相比,MBP 显示 AL 风险显著增加(OR 1.82;95%CI 1.23-2.71;p = .003)和 OM 风险增加(OR 1.38;95%CI 1.10-1.72;p = .005),oA 组所有终点均无显著差异,而 MoABP 显示 SSI 风险显著降低(OR 0.45;95%CI 0.25-0.79;p = .008)。
MoABP 可显著降低择期结直肠手术后 SSI 的风险,因此是 NBP 的有效替代方案。