Anesthesiology Department, Fundación Cardioinfantil-Instituto de Cardiología, Bogotá, Colombia.
Universidad del Rosario, Bogotá, Colombia.
J Cardiothorac Surg. 2024 Apr 17;19(1):242. doi: 10.1186/s13019-024-02722-x.
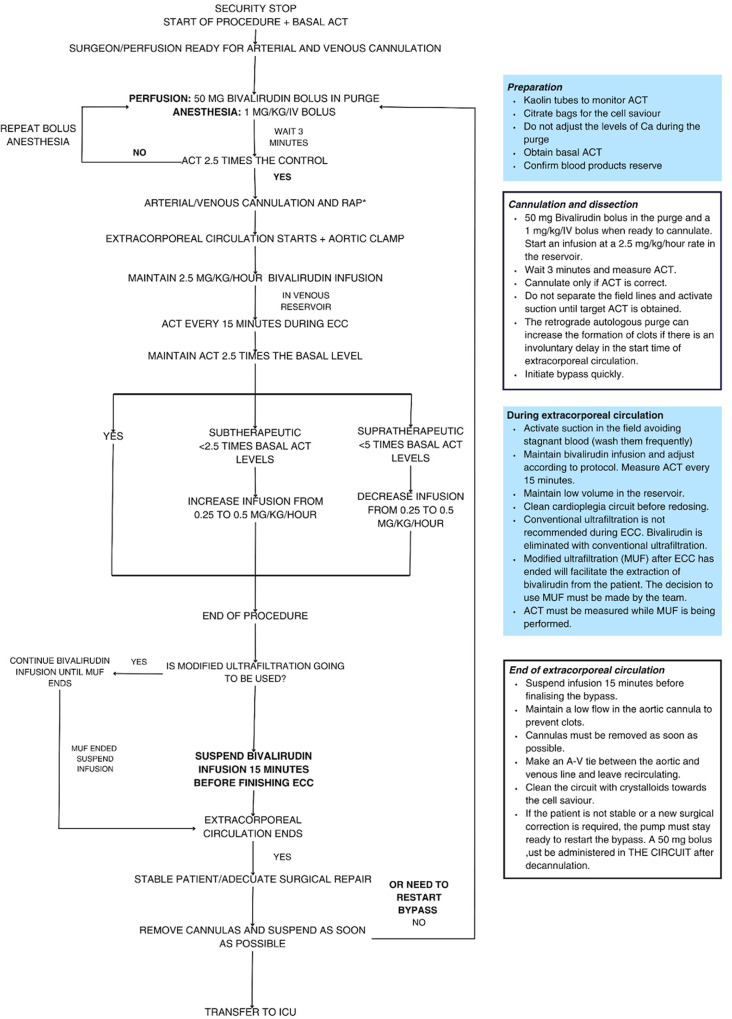
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome is a severe adverse drug reaction marked by delayed hypersensitivity reactions causing skin and systemic complications. DRESS diagnosis is challenging due to the variety of clinical presentations and symptom overlap with other conditions. The perioperative period in these patients requires precise pharmacological strategies to prevent complications associated with this syndrome. The treatment of DRESS induced by unfractionated heparin during cardiopulmonary bypass (CPB) surgery presents some challenges that must be considered when selecting an anticoagulant to avoid side effects. In this case, bivalirudin, a direct thrombin inhibitor, is indicated as an alternative to heparin in patients undergoing CPB. However, in contrast to heparin/protamine, there is no direct reversal agent for bivalirudin.
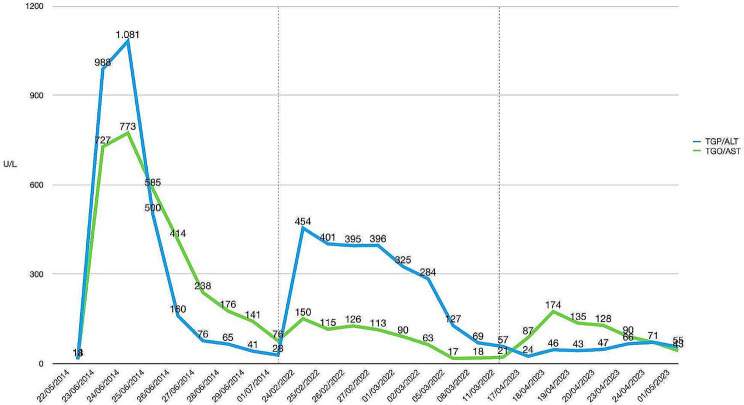
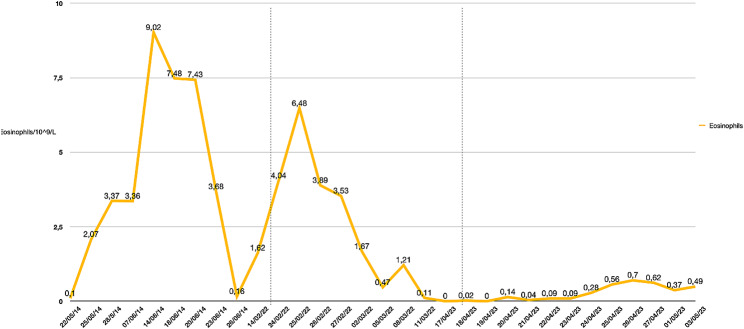
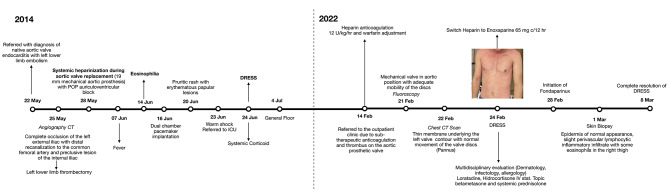
We report the case of an 11-year-old male diagnosed with native aortic valve endocarditis and thrombosis in his left lower extremity. During valvular replacement surgery, systemic unfractionated heparin was administered. Postoperatively, the patient developed fever, eosinophilia and pruritic rash. Warm shock and elevated alanine transaminase (ALT) and aspartate transaminase (AST) levels followed, leading to the diagnosis of DRESS syndrome. Treatment with methylprednisolone resulted in complete resolution of symptoms. Seven years later, the patient was readmitted due to insufficient anticoagulation and a thrombus in the prosthetic aortic valve, presenting a recurrent DRESS episode due to the administration of unfractionated heparin, which was later replaced with low-molecular-weight heparin during hospitalization. Treatment with corticosteroids and antihistamines was initiated, resulting in the resolution of this episode. Ultimately, the patient required the Ross procedure. During this intervention the anticoagulation strategy was modified, unfractionated heparin was replaced with bivalirudin during the procedure and fondaparinux was administered during the postoperative period. This resulted in stable transaminases levels and no eosinophilia.
The severity of DRESS Syndrome underscores the importance of early recognition, heightened monitoring, and a comprehensive approach tailored to each patient's needs. This particular case highlights the significance of this approach and may have a substantial clinical impact since it provides alternatives to heparin, such as bivalirudin and fondaparinux, in the anticoagulation strategy of CPB for patients who have a hypersensibility reaction to this medication; thus, enhancing clinical outcomes by minimizing risks linked to adverse drug reactions.
药物反应伴嗜酸性粒细胞增多和全身症状(DRESS)综合征是一种严重的药物不良反应,其特征为迟发性超敏反应引起皮肤和全身并发症。由于临床表现多样且与其他疾病症状重叠,DRESS 的诊断具有挑战性。这些患者的围手术期需要精确的药理学策略来预防与该综合征相关的并发症。在体外循环(CPB)手术中,由于肝素诱导的 DRESS 综合征,需要选择抗凝药物以避免副作用,这给治疗带来了一些挑战。在这种情况下,比伐卢定,一种直接凝血酶抑制剂,可作为 CPB 患者肝素的替代药物。然而,与肝素/鱼精蛋白不同,比伐卢定没有直接逆转剂。
我们报告了一例 11 岁男性患者,诊断为自体主动脉瓣心内膜炎和左下肢血栓形成。在瓣膜置换手术中,给予全身未分级肝素。术后患者出现发热、嗜酸性粒细胞增多和瘙痒性皮疹。随后出现暖休克和丙氨酸转氨酶(ALT)和天冬氨酸转氨酶(AST)水平升高,诊断为 DRESS 综合征。甲基强的松龙治疗后症状完全缓解。7 年后,由于抗凝不足和人工主动脉瓣血栓形成,患者再次入院,由于给予未分级肝素,再次出现 DRESS 发作,随后在住院期间改用低分子量肝素。开始使用皮质类固醇和抗组胺药治疗,该发作得到缓解。最终,患者需要进行罗斯手术。在该介入过程中,抗凝策略进行了修改,在手术过程中用比伐卢定代替肝素,在术后期间使用磺达肝癸钠。这导致转氨酶水平稳定且无嗜酸性粒细胞增多。
DRESS 综合征的严重程度强调了早期识别、强化监测和针对每个患者需求的综合方法的重要性。这个特殊病例突出了这种方法的重要性,并且可能具有重要的临床意义,因为它为对肝素敏感的 CPB 患者提供了肝素的替代物,如比伐卢定和磺达肝癸钠,从而通过最小化与药物不良反应相关的风险来改善临床结果。