Temoçin Fatih, Atilla Aynur, Kuruoğlu Tuba, Kamalı-Polat Ayfer
Department of Clinical Microbiology and Infectious Diseases, Ondokuz Mayıs University School of Medicine, Samsun, Turkey.
Department of General Surgery, Ondokuz Mayıs University School of Medicine, Samsun, Turkey.
Infect Dis Clin Microbiol. 2023 Mar 11;5(1):13-22. doi: 10.36519/idcm.2023.177. eCollection 2023 Mar.
Fournier's gangrene (FG) is a rare necrotizing fasciitis affecting genital and perianal areas. This study aimed to provide data on predicting factors, mortality rates, and factors affecting mortality in comparison of survivors and non-survivors in patients with FG.
This study included a retrospective analysis of patients diagnosed with FG between 2008 and 2018.
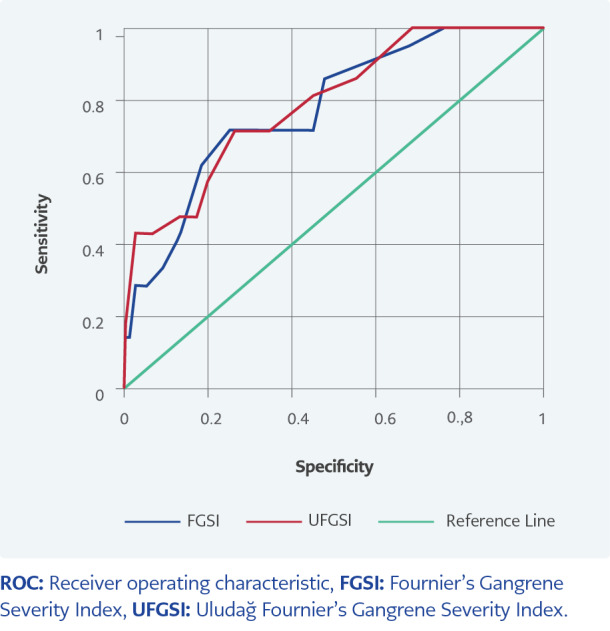
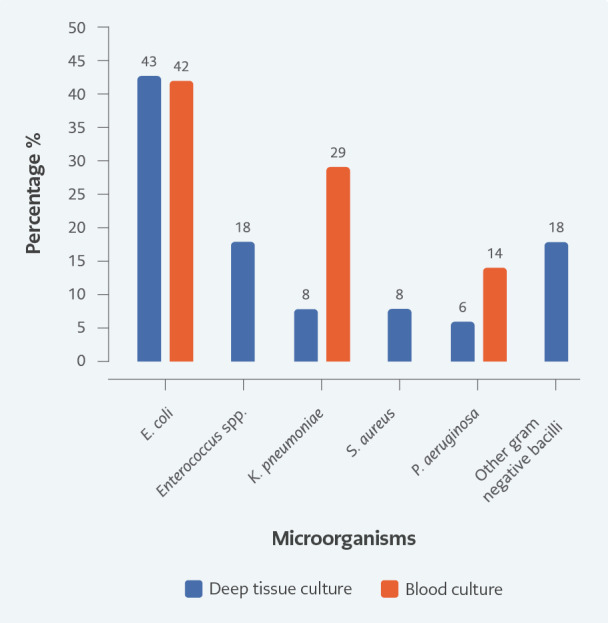
A total of 97 patients with FG were included in this study. Of the patients, 72 (74%) were male. The mean age was 56.03±13.92 years, and the median was 57 (21-90). The mortality rate was 21.6%. The most frequently isolated microorganism from tissue and blood cultures was (43%-42%). The median Fournier's Gangrene Severity Index (FGSI) and Uludağ FGSI (UFGSI) scores were 4 (0-20) and 5 (1-22), respectively. In the univariate model, mortality risk increases 7.18 times (=0.001) in patients with two or more comorbidities, 1.31 times as the FGSI score increases (<0.001), 1.28 times as the UFGSI score increases (<0.001). When the cut-off value was set as 8 for the FGSI score, the sensitivity was 71.43%, and the specificity was 73.68%. The sensitivity was 73.43%, and the specificity was 75% when the cut-off value was set as 6 for the UFGSI score. In the univariate model, the mortality risk of those with hypotension was 6.07 times higher (=0.003); as the platelet count increased, mortality risk decreased (odds ratio [OR]=0.99; =0.02). The mortality risk of those hospitalized in the intensive care unit (ICU) was 16.5 times higher than those followed in the ward (<0.001). In the multivariate model, this ratio was 6.49.
We concluded that FGSI and UFGSI scores could be used to predict mortality. Management of FG requires a multidisciplinary approach. Empiric treatment should include carbapenems and be de-escalated once getting the culture results. Authors from different centers should report their experiences to help reveal the ideal treatment and evaluate the consequences.
福尼尔坏疽(FG)是一种罕见的坏死性筋膜炎,累及生殖器和肛周区域。本研究旨在提供FG患者中预测因素、死亡率以及影响存活者与非存活者死亡率的因素的数据。
本研究纳入了2008年至2018年期间诊断为FG的患者的回顾性分析。
本研究共纳入97例FG患者。其中,72例(74%)为男性。平均年龄为56.03±13.92岁,中位数为57岁(21 - 90岁)。死亡率为21.6%。组织和血培养中最常分离出的微生物是(43% - 42%)。福尼尔坏疽严重程度指数(FGSI)和乌鲁达格FGSI(UFGSI)评分的中位数分别为4(0 - 20)和5(1 - 22)。在单变量模型中,有两种或更多合并症的患者死亡风险增加7.18倍(=0.001),FGSI评分每增加1分死亡风险增加1.31倍(<0.001),UFGSI评分每增加1分死亡风险增加1.28倍(<0.001)。当FGSI评分的截断值设定为8时,敏感性为71.43%,特异性为73.68%。当UFGSI评分的截断值设定为6时,敏感性为73.43%,特异性为75%。在单变量模型中,低血压患者的死亡风险高6.07倍(=0.003);随着血小板计数增加,死亡风险降低(比值比[OR]=0.99;=0.02)。入住重症监护病房(ICU)的患者的死亡风险比在病房接受治疗的患者高16.5倍(<0.001)。在多变量模型中,该比值为6.49。
我们得出结论,FGSI和UFGSI评分可用于预测死亡率。FG的管理需要多学科方法。经验性治疗应包括碳青霉烯类药物,并在获得培养结果后降级。不同中心的作者应报告他们的经验,以帮助揭示理想的治疗方法并评估后果。