Yönder Hüseyin, Çelik Mehmet, Berhuni Mehmet Sait, Genç Ahmed Cihad, Elkan Hasan, Tatlı Faik, Özgönül Abdullah, Çiftçi Felat, Erkmen Fırat, Karabay Oğuz, Uzunköy Ali
Department of General Surgery, Faculty of Medicine, Harran University, Şanlıurfa 63300, Turkey.
Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Harran University, Şanlıurfa 63300, Turkey.
Diagnostics (Basel). 2024 Dec 5;14(23):2732. doi: 10.3390/diagnostics14232732.
Fournier's gangrene is an aggressive, rapidly progressing, and life-threatening necrotizing fasciitis of the perineal and genital regions. Various scoring systems have been developed for predicting survival and prognosis in Fournier's gangrene. This retrospective study aimed to evaluate the effectiveness of the newly developed Fournier's gangrene mortality index (FGMI) in predicting mortality associated with Fournier's gangrene.
The study included patients over the age of 18 years who were followed-up with a diagnosis of Fournier's gangrene in the general surgery clinics of three different hospitals in Şanlıurfa province between 2014 and 2024. The patients included in this study were divided into two groups: deceased ( = 20) and surviving ( = 149). In FGMI, the parameters used were age, creatinine level, albumin level, lymphocyte percentage, and neutrophil-to-lymphocyte ratio. Based on the total score and risk assessment, <5 points were categorized as low-to-moderate mortality risk and ≥5 points as high mortality risk.
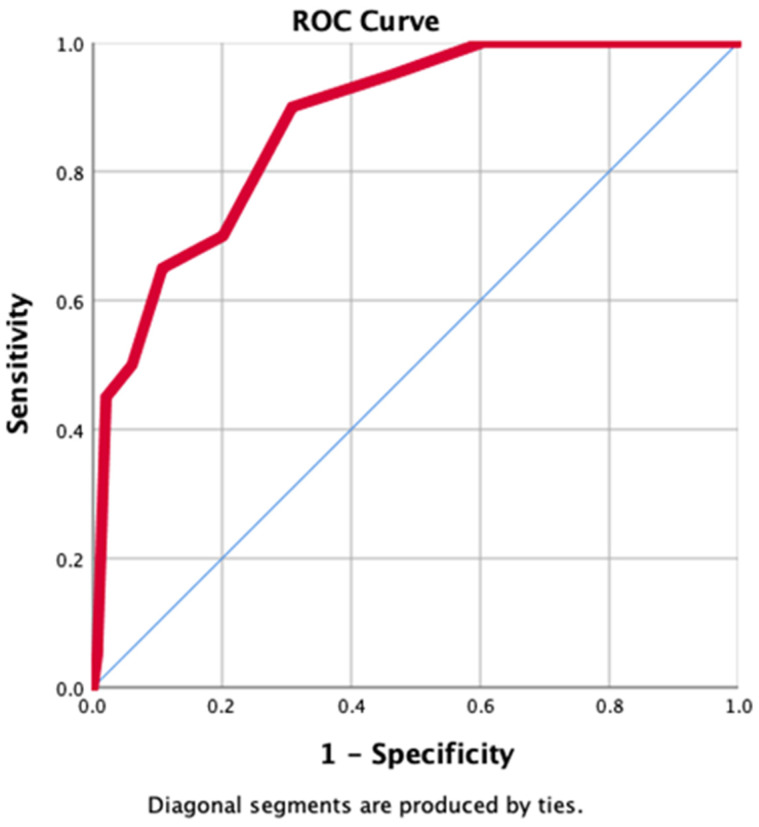
A total of 169 patients with a diagnosis of Fournier's gangrene were included in the study; 87 were men (51.48%). The median age of all patients was 53 (40-63) years; 20 patients (11.8%) died. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score did not show a statistically significant difference between the deceased and surviving groups ( = 0.5). Compared to the survivors, the deceased had higher neutrophil counts, neutrophil percentages, neutrophil-to-lymphocyte ratios, platelet-to-lymphocyte ratios, and C-reactive protein-to-albumin ratios, whereas lymphocyte counts, lymphocyte percentages, eosinophil counts, eosinophil percentages, monocyte counts, and monocyte percentages were lower, and these differences were statistically significant. According to receiver operating characteristic (ROC) analysis, the ROC-area under the curve for predicting mortality based on an FGMI score of ≥5 was 0.88 (95% CI: 0.80-0.95) with a sensitivity of 90% and a specificity of 70% ( < 0.001). Univariate risk analysis was performed, and the odds ratio revealed that mortality risk in patients followed-up for Fournier's gangrene with a FGMI score of ≥5 was 20 times higher (4.48-90.91) ( < 0.001).
The results reveal that the FGMI score is a scoring system that can predict mortality at the initial clinical presentation of patients with Fournier's gangrene. Another important finding of the present study is that the LRINEC score was not sufficiently effective in predicting mortality.
福尼尔坏疽是一种侵袭性、进展迅速且危及生命的会阴和生殖器区域坏死性筋膜炎。已经开发了各种评分系统来预测福尼尔坏疽的生存率和预后。本回顾性研究旨在评估新开发的福尼尔坏疽死亡率指数(FGMI)在预测福尼尔坏疽相关死亡率方面的有效性。
该研究纳入了2014年至2024年期间在Şanlıurfa省三家不同医院的普通外科诊所被诊断为福尼尔坏疽并接受随访的18岁以上患者。本研究纳入的患者分为两组:死亡组(=20)和存活组(=149)。在FGMI中,使用的参数为年龄、肌酐水平、白蛋白水平、淋巴细胞百分比和中性粒细胞与淋巴细胞比值。根据总分和风险评估,<5分为低至中度死亡风险,≥5分为高死亡风险。
本研究共纳入169例诊断为福尼尔坏疽的患者;87例为男性(51.48%)。所有患者的中位年龄为53(40 - 63)岁;20例患者(11.8%)死亡。坏死性筋膜炎实验室风险指标(LRINEC)评分在死亡组和存活组之间未显示出统计学显著差异(=0.5)。与存活者相比,死亡者的中性粒细胞计数、中性粒细胞百分比、中性粒细胞与淋巴细胞比值、血小板与淋巴细胞比值以及C反应蛋白与白蛋白比值更高,而淋巴细胞计数、淋巴细胞百分比、嗜酸性粒细胞计数、嗜酸性粒细胞百分比、单核细胞计数和单核细胞百分比更低,且这些差异具有统计学意义。根据受试者工作特征(ROC)分析,基于FGMI评分≥5预测死亡率的曲线下面积为0.88(95%CI:0.80 - 0.95),敏感性为90%,特异性为70%(<0.001)。进行了单因素风险分析,比值比显示FGMI评分≥5的福尼尔坏疽随访患者的死亡风险高20倍(4.48 - 90.91)(<0.001)。
结果表明,FGMI评分是一种能够在福尼尔坏疽患者初始临床表现时预测死亡率的评分系统。本研究的另一个重要发现是,LRINEC评分在预测死亡率方面不够有效。