Division of Pulmonary and Critical Care Medicine, Department of Medicine, University of Michigan, Ann Arbor.
VA Center for Clinical Management Research, Ann Arbor, Michigan.
JAMA Netw Open. 2024 Apr 1;7(4):e247480. doi: 10.1001/jamanetworkopen.2024.7480.
Recent sepsis trials suggest that fluid-liberal vs fluid-restrictive resuscitation has similar outcomes. These trials used generalized approaches to resuscitation, and little is known about how clinicians personalize fluid and vasopressor administration in practice.
To understand how clinicians personalize decisions about resuscitation in practice.
DESIGN, SETTING, AND PARTICIPANTS: This survey study of US clinicians in the Society of Critical Care Medicine membership roster was conducted from November 2022 to January 2023. Surveys contained 10 vignettes of patients with sepsis where pertinent clinical factors (eg, fluid received and volume status) were randomized. Respondents selected the next steps in management. Data analysis was conducted from February to September 2023.
Online Qualtrics clinical vignette survey.
Using multivariable logistic regression, the associations of clinical factors with decisions about fluid administration, vasopressor initiation, and vasopressor route were tested. Results are presented as adjusted proportions with 95% CIs.
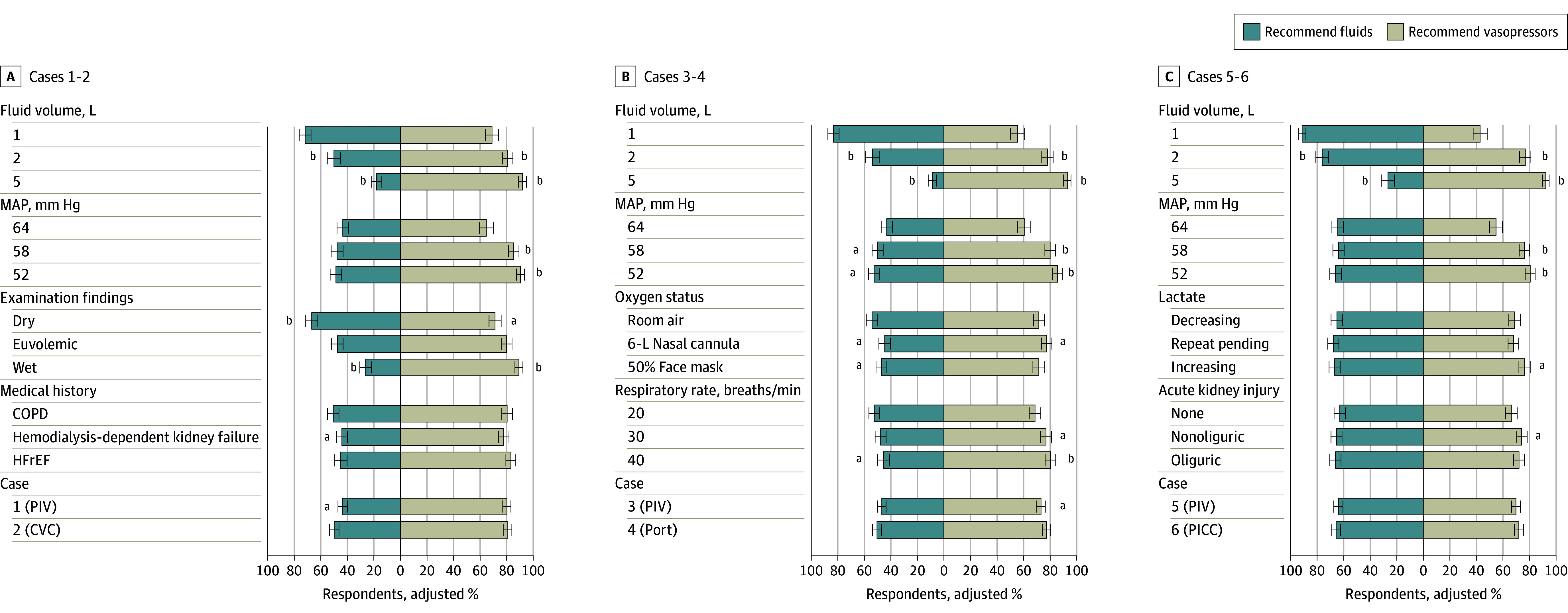
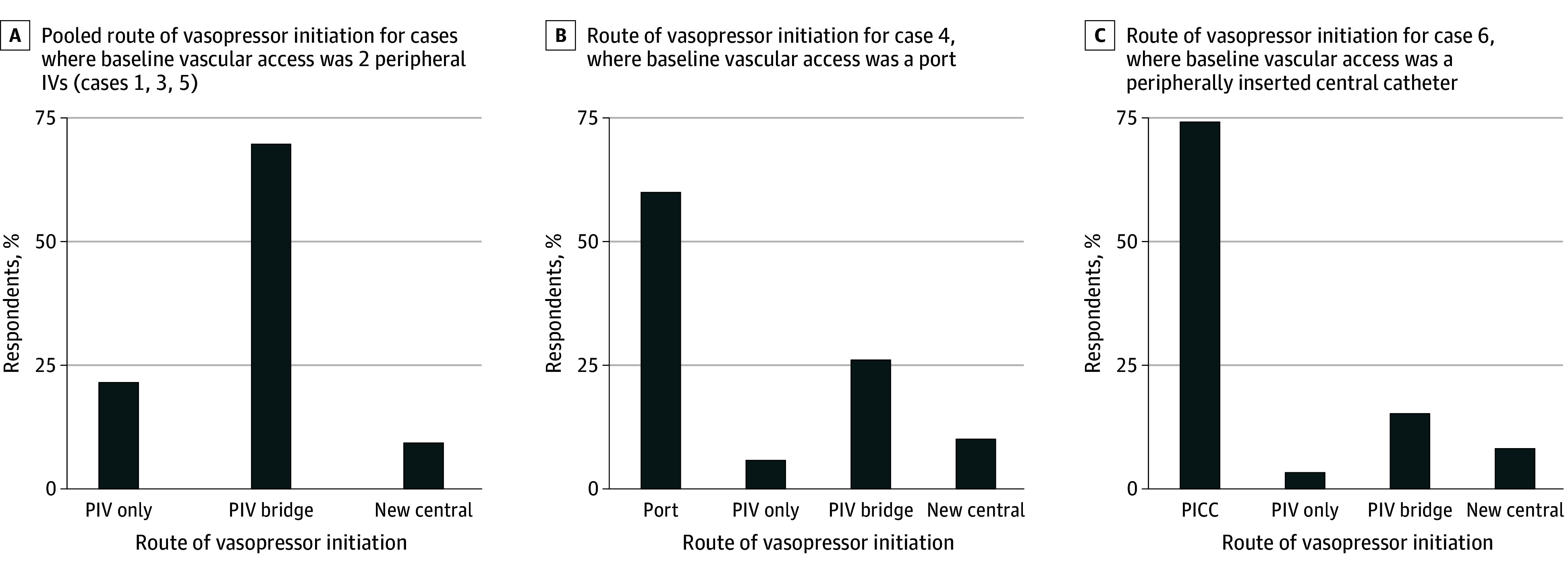
Among 11 203 invited clinicians, 550 (4.9%; 261 men [47.5%] and 192 women [34.9%]; 173 with >15 years of practice [31.5%]) completed at least 1 vignette and were included. A majority were physicians (337 respondents [61.3%]) and critical care trained (369 respondents [67.1%]). Fluid volume already received by a patient was associated with resuscitation decisions. After 1 L of fluid, an adjusted 82.5% (95% CI, 80.2%-84.8%) of respondents prescribed additional fluid and an adjusted 55.0% (95% CI, 51.9%-58.1%) initiated vasopressors. After 5 L of fluid, an adjusted 17.5% (95% CI, 15.1%-19.9%) of respondents prescribed more fluid while an adjusted 92.7% (95% CI, 91.1%-94.3%) initiated vasopressors. More respondents prescribed fluid when the patient examination found dry vs wet (ie, overloaded) volume status (adjusted proportion, 66.9% [95% CI, 62.5%-71.2%] vs adjusted proportion, 26.5% [95% CI, 22.3%-30.6%]). Medical history, respiratory status, lactate trend, and acute kidney injury had small associations with fluid and vasopressor decisions. In 1023 of 1127 vignettes (90.8%) where the patient did not have central access, respondents were willing to start vasopressors through a peripheral intravenous catheter. In cases where patients were already receiving peripheral norepinephrine, respondents were more likely to place a central line at higher norepinephrine doses of 0.5 µg/kg/min (adjusted proportion, 78.0%; 95% CI, 74.7%-81.2%) vs 0.08 µg/kg/min (adjusted proportion, 25.2%; 95% CI, 21.8%-28.5%) and after 24 hours (adjusted proportion, 59.5%; 95% CI, 56.6%-62.5%) vs 8 hours (adjusted proportion, 47.1%; 95% CI, 44.0%-50.1%).
These findings suggest that fluid volume received is the predominant factor associated with ongoing fluid and vasopressor decisions, outweighing many other clinical factors. Peripheral vasopressor use is common. Future studies aimed at personalizing resuscitation must account for fluid volumes and should incorporate specific tools to help clinicians personalize resuscitation.
最近的脓毒症试验表明,液体自由复苏与液体限制复苏具有相似的结果。这些试验采用了通用的复苏方法,对于临床医生在实践中如何个性化地管理液体和血管加压剂的使用知之甚少。
了解临床医生在实践中如何个性化地做出复苏决策。
设计、地点和参与者:这项对美国重症监护医学学会会员名单中的临床医生进行的调查研究于 2022 年 11 月至 2023 年 1 月进行。调查包含了 10 个脓毒症患者的病例,其中相关的临床因素(例如,接受的液体量和容量状态)是随机的。受访者选择下一步的治疗方案。数据分析于 2023 年 2 月至 9 月进行。
在线 Qualtrics 临床病例调查。
使用多变量逻辑回归,检验了临床因素与液体管理、血管加压剂启动和血管加压剂途径决策的关联。结果以调整后的比例(95%CI)呈现。
在邀请的 11203 名临床医生中,有 550 名(4.9%;261 名男性[47.5%]和 192 名女性[34.9%];173 名具有>15 年实践经验[31.5%])至少完成了 1 个病例并被纳入分析。大多数是医生(337 名受访者[61.3%])和重症监护培训医生(369 名受访者[67.1%])。患者已经接受的液体量与复苏决策相关。在接受 1 L 液体后,调整后的 82.5%(95%CI,80.2%-84.8%)的受访者开了更多的液体,调整后的 55.0%(95%CI,51.9%-58.1%)的受访者开始使用血管加压剂。在接受 5 L 液体后,调整后的 17.5%(95%CI,15.1%-19.9%)的受访者开了更多的液体,而调整后的 92.7%(95%CI,91.1%-94.3%)的受访者开始使用血管加压剂。当患者检查发现干(即超负荷)和湿(即容量过载)容量状态时,更多的受访者开了液体(调整后的比例,66.9%[95%CI,62.5%-71.2%]与调整后的比例,26.5%[95%CI,22.3%-30.6%])。医疗史、呼吸状况、乳酸趋势和急性肾损伤与液体和血管加压剂决策有较小的关联。在 1127 个病例中的 1023 个(90.8%)患者没有中心通路的情况下,受访者愿意通过外周静脉导管开始使用血管加压剂。在患者已经接受外周去甲肾上腺素的情况下,当患者的去甲肾上腺素剂量更高(0.5 µg/kg/min)时,受访者更有可能放置中心静脉导管(调整后的比例,78.0%[95%CI,74.7%-81.2%]与 0.08 µg/kg/min(调整后的比例,25.2%[95%CI,21.8%-28.5%])和 24 小时后(调整后的比例,59.5%[95%CI,56.6%-62.5%]与 8 小时后(调整后的比例,47.1%[95%CI,44.0%-50.1%])。
这些发现表明,接受的液体量是与持续液体和血管加压剂决策相关的主要因素,超过了许多其他临床因素。外周血管加压剂的使用很常见。未来旨在个性化复苏的研究必须考虑到液体量,并应纳入特定的工具来帮助临床医生个性化复苏。