Xavier Tiago Batista, Coelho Leonardo Vicente, Ferreira Daniel Antonio Lopes, Cota Y Raposeiras José Manuel, Duran Marcelo Sampaio, Silva Leticia Almeida, da Motta-Ribeiro Gabriel Casulari, Camilo Luciana Moisés, Carvalho Alysson Roncally Silva, Silva Pedro Leme
Laboratório de Fisiologia da Respiração, Instituto de Biofísica Carlos Chagas Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil.
Instituto de Educação, Ciência e Tecnologia do Rio de Janeiro, Rio de Janeiro, Brazil.
Front Physiol. 2024 Apr 5;15:1383167. doi: 10.3389/fphys.2024.1383167. eCollection 2024.
During pneumoperitoneum (PNP), airway driving pressure (ΔP) increases due to the stiffness of the chest wall and cephalic shift of the diaphragm, which favors atelectasis. In addition, depending on the mechanical power (MP) formulas, they may lead to different interpretations.
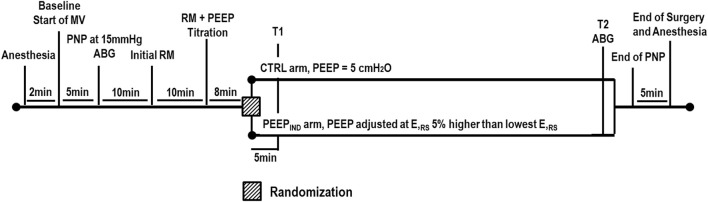
Patients >18 years of age with body mass index >35 kg/m were included in a single-center randomized controlled trial during their admission for bariatric surgery by abdominal laparoscopy. Intra-abdominal pressure was set at 15 mmHg at the pneumoperitoneum time point (PNP). After the recruitment maneuver, the lowest respiratory system elastance (E) was detected during the positive end-expiratory pressure (PEEP) step-wise decrement. Patients were randomized to the 1) CTRL group: ventilated with PEEP of 5 cmHO and 2) PEEP group: ventilated with PEEP value associated with E that is 5% higher than its lowest level. Respiratory system mechanics and mean arterial pressure (MAP) were assessed at the PNP, 5 min after randomization (T1), and at the end of the ventilation protocol (T2); arterial blood gas was assessed at PNP and T2. ΔP was the primary outcome. Three MP formulas were used: MP, which computes static PEEP × volume, elastic, and resistive components; MP, which computes only the elastic component; and MP, which computes static PEEP × volume, elastic, and resistive components without inspiratory holds.
Twenty-eight patients were assessed for eligibility: eight were not included and 20 patients were randomized and allocated to CTRL and PEEP groups ( = 10/group). The PEEP ventilator strategy reduced ΔP when compared with the CTRL group (PEEP, 13 ± 2 cmHO; CTRL, 22 ± 4 cmHO; < 0.001). Oxygenation improved in the PEEP group when compared with the CTRL group ( = 0.029), whereas MAP was comparable between the PEEP and CTRL groups. At the end of surgery, MP and MP were correlated in both the CTRL (rho = 0.71, = 0.019) and PEEP (rho = 0.84, = 0.020) groups but showed different bias (CTRL, -1.9 J/min; PEEP, +10.0 J/min). At the end of the surgery, MP and MP were correlated in both the CTRL (rho = 0.71, = 0.019) and PEEP (rho = 0.84, = 0.020) groups but showed different bias (CTRL, -1.9 J/min; PEEP, +10.0 J/min).
Individualized PEEP was associated with a reduction in ΔP and an improvement in oxygenation with comparable MAP. The MP, which solely computes the elastic component, better reflected the improvement in ΔP observed in the individualized PEEP group.
The protocol was registered at the Brazilian Registry of Clinical Trials (U1111-1220-7296).
在气腹(PNP)期间,由于胸壁僵硬和膈肌头侧移位,气道驱动压(ΔP)会升高,这有利于肺不张的发生。此外,根据机械功率(MP)公式,可能会导致不同的解读。
年龄>18岁、体重指数>35kg/m²的患者在接受腹腔镜减肥手术入院期间被纳入一项单中心随机对照试验。气腹时间点(PNP)时腹内压设定为15mmHg。在进行肺复张手法后,在呼气末正压(PEEP)逐步降低过程中检测到最低呼吸系统弹性(E)。患者被随机分为1)对照组:采用5cmH₂O的PEEP进行通气;2)PEEP组:采用与E相关的PEEP值进行通气,该值比其最低水平高5%。在PNP、随机分组后5分钟(T1)和通气方案结束时(T2)评估呼吸系统力学和平均动脉压(MAP);在PNP和T2时评估动脉血气。ΔP是主要结局。使用了三种MP公式:计算静态PEEP×容积、弹性和阻力成分的MP;仅计算弹性成分的MP;以及不进行吸气暂停计算静态PEEP×容积、弹性和阻力成分的MP。
评估了28例患者的 eligibility:8例未纳入,20例患者被随机分组并分配到对照组和PEEP组(每组 = 10例)。与对照组相比,PEEP通气策略降低了ΔP(PEEP组为13±2cmH₂O;对照组为22±4cmH₂O;P<0.001)。与对照组相比,PEEP组的氧合改善(P = 0.029),而PEEP组和对照组之间的MAP相当。手术结束时,对照组(rho = 0.71,P = 0.019)和PEEP组(rho = 0.84,P = 0.020)中MP和MP均相关,但显示出不同的偏差(对照组为-1.9J/min;PEEP组为+10.0J/min)。手术结束时,对照组(rho = 0.71,P = 0.019)和PEEP组(rho = 0.84,P = 0.020)中MP和MP均相关,但显示出不同的偏差(对照组为-1.9J/min;PEEP组为+10.0J/min)。
个体化PEEP与ΔP降低和氧合改善相关,且MAP相当。仅计算弹性成分的MP能更好地反映个体化PEEP组中观察到的ΔP改善情况。
该方案已在巴西临床试验注册中心注册(U1111-1220-7296)。