Princess Máxima Center for Pediatric Oncology, Utrecht, the Netherlands.
Cansearch Research Platform for Pediatric Oncology and Hematology, Faculty of Medicine, Department of Pediatrics, Gynecology and Obstetrics, University of Geneva, Division of Pediatric Oncology and Hematology, Department of Women, Child and Adolescent, University Geneva Hospitals, Geneva, Switzerland.
J Clin Oncol. 2024 Jun 20;42(18):2219-2232. doi: 10.1200/JCO.23.02353. Epub 2024 Apr 22.
Hearing loss occurs in 50%-70% of children treated with cisplatin. Scientific efforts have led to the recent approval of a pediatric formula of intravenous sodium thiosulfate (STS) for otoprotection by the US Food and Drug Administration, the European Medicines Agency, and the Medicines and Health Regulatory Authority in the United Kingdom. To inform stakeholders regarding the clinical utility of STS, the current review summarizes available literature on the efficacy, pharmacokinetics (PK), and safety of systemic STS to minimize cisplatin-induced hearing loss (CIHL).
A comprehensive narrative review is presented.
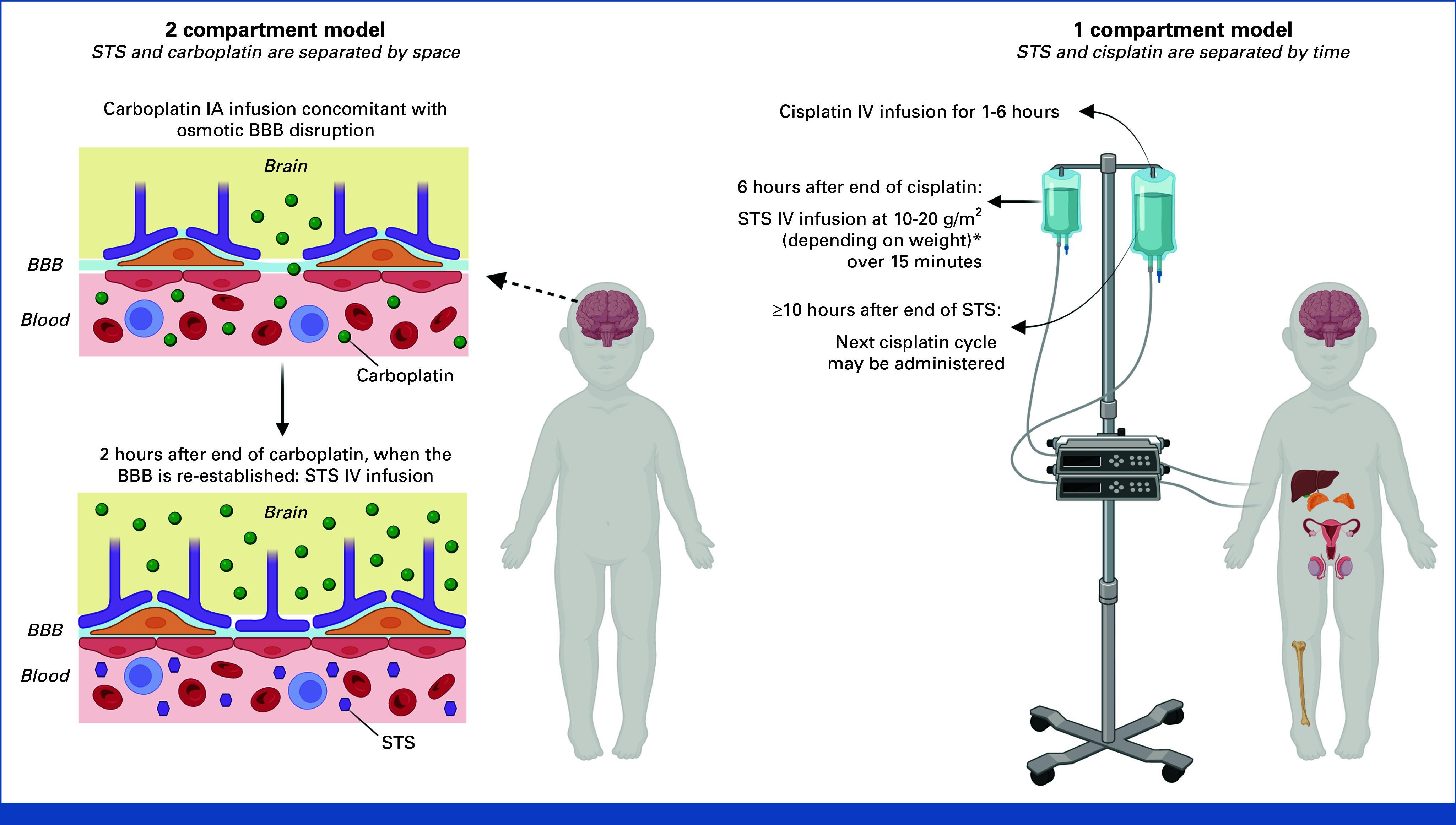
Thirty-one articles were summarized. Overall, systemic STS effectively reduces CIHL in the preclinical and controlled clinical study settings, in both adults and children with cancer. The extent of CIHL reduction depends on the timing and dosing of STS in relation to cisplatin. Both preclinical and clinical data suggest that systemic STS may affect plasma platinum levels, but studies are inconclusive. Delayed systemic administration of STS, at 6 hours after the cisplatin infusion, does not affect cisplatin-induced inhibition of tumor growth or cellular cytotoxicity in the preclinical setting, nor affect cisplatin efficacy and survival in children with localized disease in the clinical setting.
Systemic administration of STS effectively reduces the development and degree of CIHL in both the preclinical and clinical settings. More studies are needed on the PK of STS and cisplatin drug combinations, the efficacy and safety of STS in patients with disseminated disease, and the ability of STS to prevent further deterioration of pre-established hearing loss.
顺铂治疗的儿童中有 50%-70%发生听力损失。科学研究促使美国食品和药物管理局、欧洲药品管理局和英国药品和保健产品监管局最近批准了一种小儿静脉注射硫代硫酸钠(STS)配方,用于耳保护。为了向利益相关者通报 STS 的临床实用性,本综述总结了关于全身 STS 的疗效、药代动力学(PK)和安全性的现有文献,以最大限度地减少顺铂引起的听力损失(CIHL)。
呈现了全面的叙述性综述。
总结了 31 篇文章。总的来说,全身 STS 在临床前和对照临床试验中有效降低了癌症成人和儿童的 CIHL。CIHL 减少的程度取决于 STS 与顺铂的时间和剂量。临床前和临床数据均表明,全身 STS 可能会影响血浆铂水平,但研究尚无定论。STS 的延迟全身给药,即在顺铂输注后 6 小时给予 STS,不会影响临床前环境中顺铂对肿瘤生长或细胞细胞毒性的抑制作用,也不会影响局部疾病儿童的顺铂疗效和生存。
全身 STS 给药可有效降低临床前和临床环境中 CIHL 的发生和程度。需要更多关于 STS 和顺铂药物组合的 PK、STS 在播散性疾病患者中的疗效和安全性以及 STS 预防已建立的听力损失进一步恶化的能力的研究。