Guangdong Key Laboratory of Age-Related Cardiac and Cerebral Diseases, Affiliated Hospital of Guangdong Medical University, Zhanjiang, China.
Department of Neurology, Affiliated Hospital of Guangdong Medical University, Zhanjiang, 524000, China.
BMC Neurol. 2024 Apr 25;24(1):140. doi: 10.1186/s12883-024-03617-z.
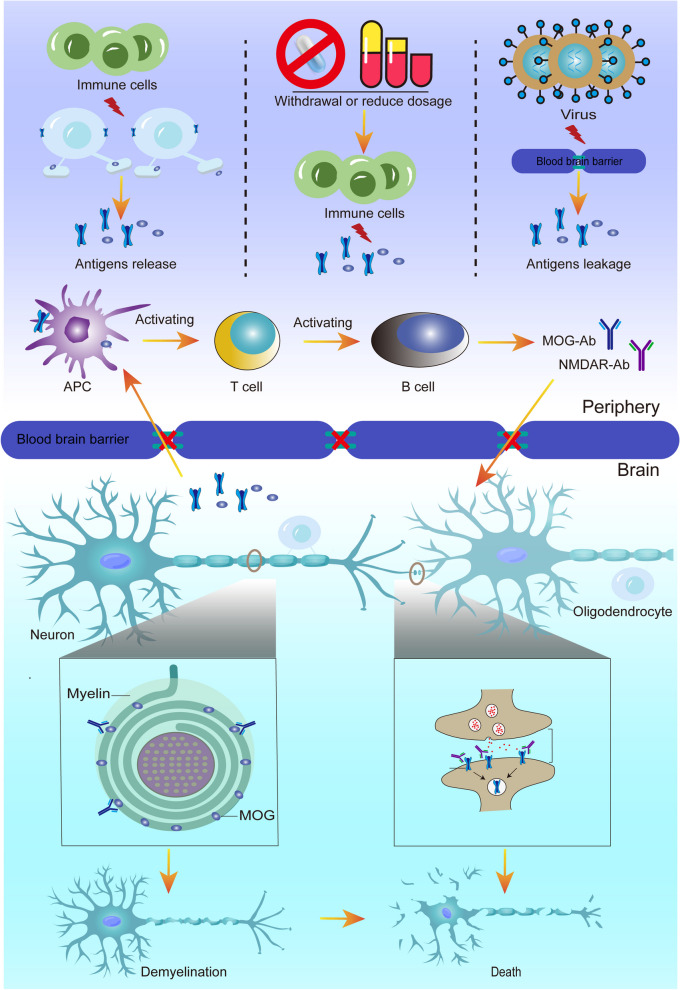
In recent years, simultaneous or sequential occurrence of MOG antibody disease and anti-NMDAR encephalitis in the same patient has been reported with increasing frequency. Scholars refer to the overlapping occurrence of these two disorders as MOG antibody disease and anti-NMDAR encephalitis overlap syndrome (MNOS). Cortical T2-weighted fluid-attenuated inversion recovery (FLAIR) -hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES) is a rare clinical phenotype of MOGAD in which cortical FLAIR high-signal lesions are unilateral, with little spread to the cortex and meninges bilaterally. Although cases of FLAMES have been consistently reported. However, to our knowledge, such cases of FLAMES combined with NMDARE are rare.
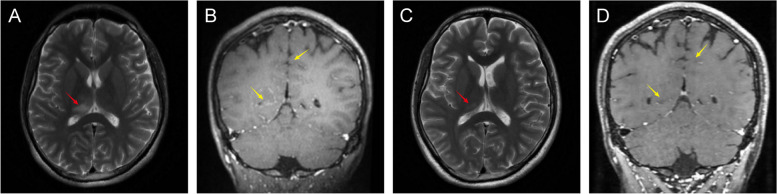
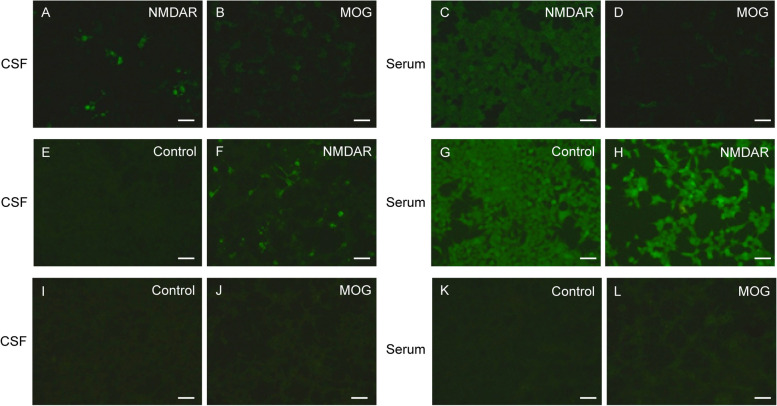
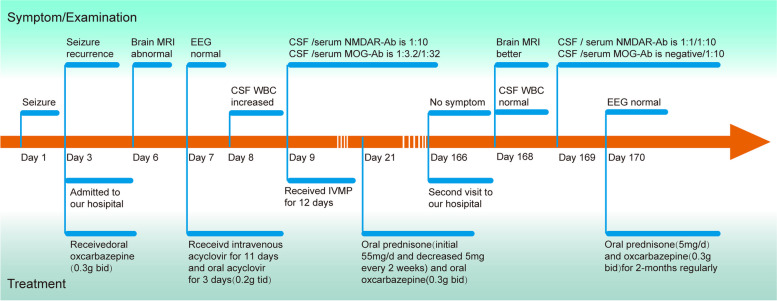
Here, we describe a case of FLAMES combined with anti-NMDARE. The patient was a young male, 29 years old, admitted to our hospital with isolated seizures, whose MRI showed unilateral thalamic and bilateral frontal and parietal leptomeningeal involvement. Since we were unaware of the possibility of bilateral meningo-cortical MOGAD manifestations, the case was initially diagnosed as viral encephalitis and was given antiviral therapy. The diagnosis was not clarified until anti-NMDAR-IgG and MOG-IgG positivity was detected in the cerebrospinal fluid and serum. The patient was then treated with high-dose corticosteroids and his symptoms responded well to the steroids. Therefore, this case expands the clinical spectrum of MNOS overlap syndrome. In addition, we describe the clinical features of MNOS by summarizing the existing literature and exploring the possible mechanisms of its immune response.
Our case serves as a reminder to clinicians that when patients present with atypical clinical manifestations such as seizures, consideration should be given to MNOS and conduct testing for various relevant autoantibodies (including MOG abs) and viruses in both serum and cerebrospinal fluid, as it is easy to misdiagnose the disease as other CNS diseases, such as viral meningoencephalitis. This syndrome exhibits a high responsiveness to steroids, highlighting the critical importance of recognizing the clinical and neuroimaging features of this overlap syndrome for prompt diagnosis and treatment. Furthermore, it enriches the disease spectrum of MNOS.
近年来,越来越多的病例报告显示,MOG 抗体病和抗 NMDAR 脑炎在同一患者中同时或序贯发生。学者们将这两种疾病的重叠发生称为 MOG 抗体病和抗 NMDAR 脑炎重叠综合征(MNOS)。伴有癫痫发作的抗 MOG 相关脑炎的皮质 T2 加权液体衰减反转恢复(FLAIR)高信号病变(FLAMES)是 MOAD 的一种罕见临床表型,其皮质 FLAIR 高信号病变单侧,很少扩散到双侧皮质和脑膜。虽然一直有报道称存在 FLAMES 病例,但据我们所知,同时存在 FLAMES 和 NMDARE 的病例非常罕见。
本病例报告了一例同时存在 FLAMES 和抗 NMDARE 的病例。患者为 29 岁年轻男性,因孤立性癫痫发作入院,其 MRI 显示单侧丘脑和双侧额顶叶脑膜受累。由于我们不知道可能存在双侧脑膜-皮质 MOGAD 表现,因此最初将该病例诊断为病毒性脑炎,并给予抗病毒治疗。直到在脑脊液和血清中检测到抗 NMDAR-IgG 和 MOG-IgG 阳性后,才明确诊断。随后,该患者接受了大剂量皮质类固醇治疗,症状对类固醇反应良好。因此,该病例扩大了 MNOS 重叠综合征的临床谱。此外,我们通过总结现有文献并探讨其免疫反应的可能机制,描述了 MNOS 重叠综合征的临床特征。
本病例提醒临床医生,当患者出现癫痫等非典型临床表现时,应考虑 MNOS,并对血清和脑脊液中的各种相关自身抗体(包括 MOG abs)和病毒进行检测,因为很容易将该疾病误诊为其他 CNS 疾病,如病毒性脑膜脑炎。该综合征对类固醇反应良好,突出了认识该重叠综合征的临床和神经影像学特征对于及时诊断和治疗的重要性。此外,它丰富了 MNOS 的疾病谱。