Nitta Toshikatsu, Yoshioka Shinichi, Ishii Masatsugu, Taki Masataka, Kubo Ryutaro, Ishibashi Takashi
Division of Surgery, Gastroenterological Center, Medico Shunju Shiroyama Hospital, Osaka, Japan; Department of Surgery, Gastroenterological Surgery, Yao Municipal Hospital, Osaka, Japan.
Division of Surgery, Gastroenterological Center, Medico Shunju Shiroyama Hospital, Osaka, Japan; Department of Surgery, Gastroenterological Surgery, Yao Municipal Hospital, Osaka, Japan.
Int J Surg Case Rep. 2024 May;118:109693. doi: 10.1016/j.ijscr.2024.109693. Epub 2024 Apr 24.
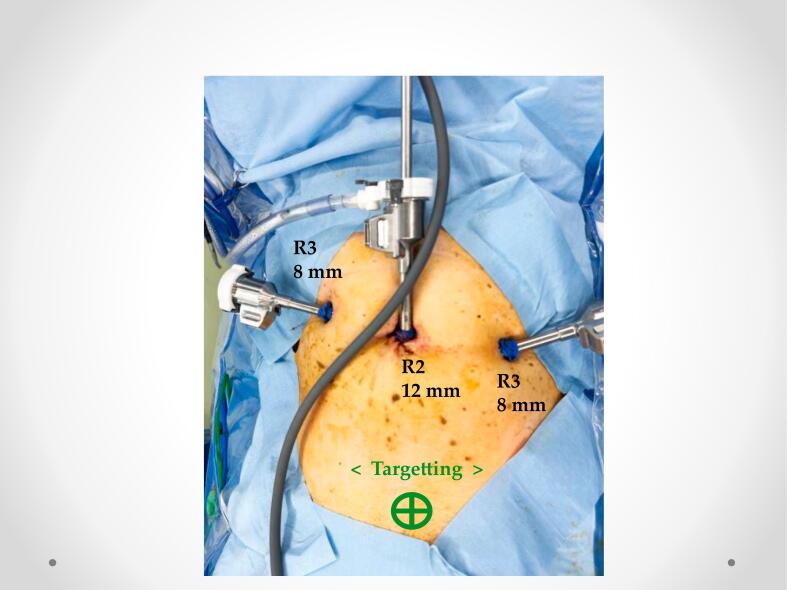
The laparoscopic posterior approach adapts the advantages of Kugel hernioplasty, making it possible to perform it at the new layer even if the inguinal hernia is recurrent following the anterior approach, producing a high level of completion. However, in laparoscopic surgery for recurrent inguinal hernia using posterior approaches, dissecting the extraperitoneal space is difficult. Robotic surgery may enable precise dissection, even if the space is severely adhered. Here, we report a robotic approach after extraperitoneal approach for recurrent inguinal hernia, which developed after Kugel hernioplasty.
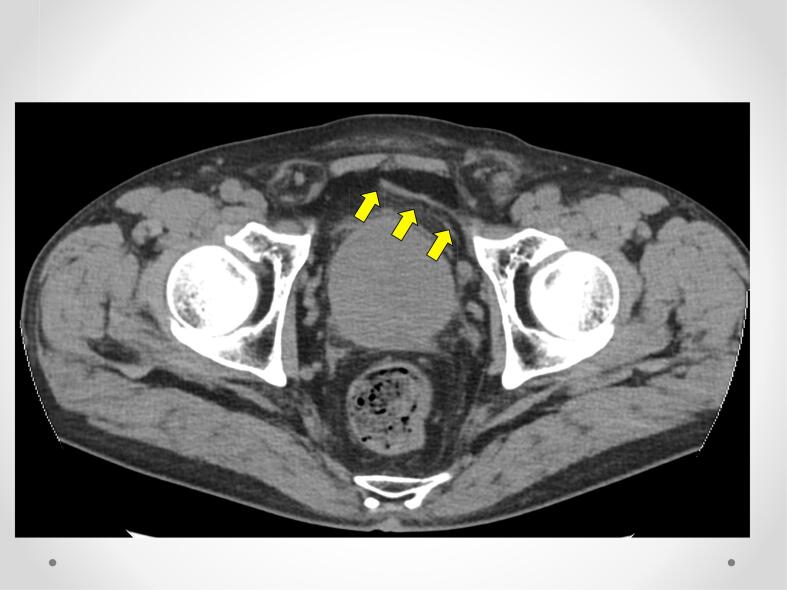
A 78-year-old Japanese man, who underwent left inguinal hernia repair (Kugel hernioplasty) 2 years ago, presented with recurrent reducible left inguinal swelling. A peritoneal incision was created above the deep inguinal ring to treat the primary right inguinal hernia. The pressure in the left inguinal region revealed a spermatic cord lipoma protruding from the internal inguinal ring as a recurrent inguinal hernia of the abdominal cavity.
Robotic transabdominal preperitoneal repair for recurrent inguinal hernia is effective, especially after posterior approach Kugel hernioplasty, in which dissection of the extraperitoneal space is difficult. In the present case, the peritoneal flap was conserved without removing the direct Kugel patch.
Kugel hernioplasty, which is a posterior approach, would result in severe extraperitoneal space adhesion. Essentially, a new and previously unused approach is preferable to the previous approach in patients with recurrent inguinal hernias. Robotic approach is effective for recurrent inguinal hernias even if the space was severe adhesion.
腹腔镜后路手术融合了库格尔疝修补术的优点,即使腹股沟疝在前路手术后复发,也能够在新层次进行手术,完成度较高。然而,在采用后路手术的复发性腹股沟疝腹腔镜手术中,解剖腹膜外间隙较为困难。机器人手术即便在该间隙严重粘连的情况下也可能实现精确解剖。在此,我们报告一例在库格尔疝修补术后出现的复发性腹股沟疝经腹膜外途径后的机器人手术方法。
一名78岁的日本男性,2年前接受了左侧腹股沟疝修补术(库格尔疝修补术),现出现左侧腹股沟可复性肿胀复发。在腹股沟深环上方做腹膜切口以治疗原发性右侧腹股沟疝。左侧腹股沟区压力检查显示,有一个精索脂肪瘤从腹股沟内环突出,为腹腔复发性腹股沟疝。
机器人经腹腹膜前修补复发性腹股沟疝是有效的,特别是在库格尔疝修补术后路手术中,此时解剖腹膜外间隙困难。在本病例中,保留了腹膜瓣,未移除直接的库格尔补片。
库格尔疝修补术作为一种后路手术,会导致腹膜外间隙严重粘连。本质上,对于复发性腹股沟疝患者,一种新的且此前未使用过的手术方法优于先前的方法。即使间隙严重粘连,机器人手术对于复发性腹股沟疝也是有效的。