Voldby Anders W, Aaen Anne A, Møller Ann M, Brandstrup Birgitte
Department of Surgery, Holbæk Hospital, Part of Copenhagen University Hospitals, Smedelundsgade 60, 4300, Holbaek, Denmark.
Department of Anesthesiology and Intensive Care Medicine, Holbæk Hospital, Smedelundsgade 60, 4300, Holbaek, Denmark.
Perioper Med (Lond). 2024 Apr 26;13(1):32. doi: 10.1186/s13741-024-00390-y.
The association between perioperative fluid administration and risk of complications following emergency surgery is poorly studied. We tested the association between the perioperative fluid balance and postoperative complications following emergency surgery for gastrointestinal obstruction or perforation.
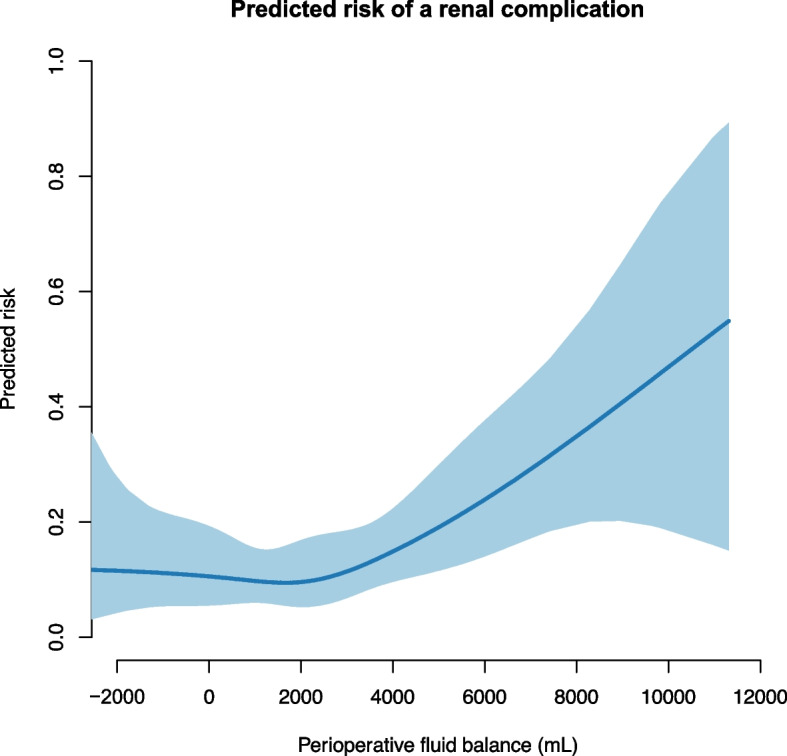
We performed a re-assessment of data from the Goal-directed Fluid Therapy in Urgent Gastrointestinal Surgery Trial (GAS-ART) studying intra-operative stroke volume optimization and postoperative zero-balance fluid therapy versus standard fluid therapy. The cohort was divided into three groups at a perioperative fluid balance (FB) of low < 0 L, moderate 0-2 L, or high > 2 L. We used a propensity adjusted logistic regression to analyse the association with cardiopulmonary (primary outcome), renal, infectious, and wound healing complications. Further, the risk of complications was explored on a continuous scale of the FB.
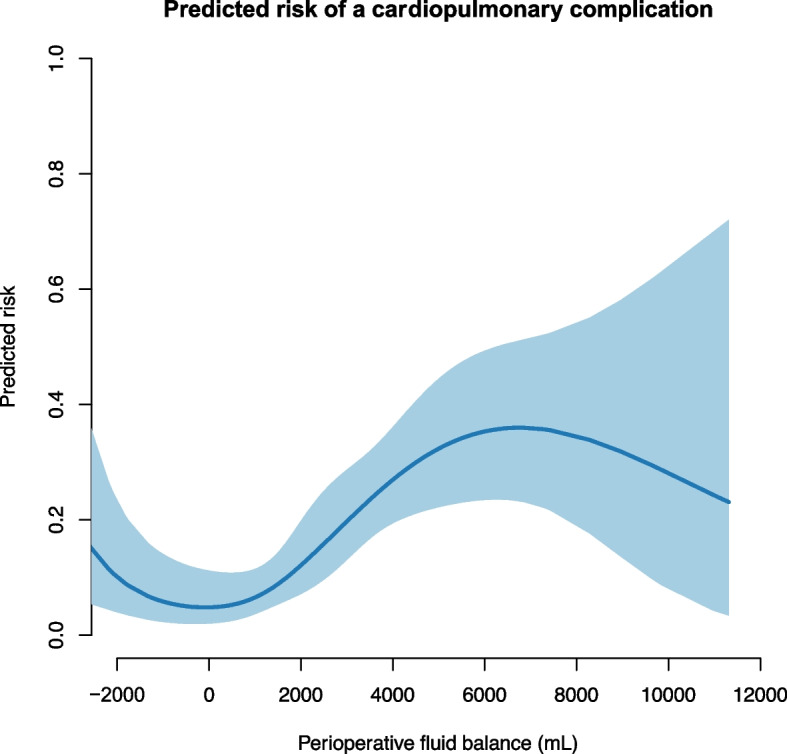
We included 303 patients: 44 patients belonged to the low-FB group, 108 to the moderate-FB group, and 151 to the high-FB group. The median [interquartile range] perioperative FB was -0.9 L [-1.4, -0.6], 0.9 L [0.5, 1.3], and 3.8 L [2.7, 5.3]. The risk of cardiopulmonary complications was significantly higher in the High-FB group 3.4 (1.5-7.6), p = 0.002 (odds ratio (95% confidence interval). On a continuous scale of the fluid balance, the risk of cardiopulmonary complications was minimal at -1 L to 1 L.
Following emergency surgery for gastrointestinal obstruction or perforation, a fluid balance < 2.0 L was associated with decreased risk of cardiopulmonary complications without increasing renal complications.
围手术期液体输注与急诊手术后并发症风险之间的关联研究较少。我们测试了胃肠道梗阻或穿孔急诊手术后围手术期液体平衡与术后并发症之间的关联。
我们对“紧急胃肠手术目标导向液体治疗试验”(GAS-ART)的数据进行了重新评估,该试验研究术中每搏量优化和术后零平衡液体治疗与标准液体治疗的对比。根据围手术期液体平衡(FB)将队列分为三组:低FB组<0L、中FB组0-2L或高FB组>2L。我们使用倾向调整逻辑回归分析与心肺(主要结局)、肾脏、感染和伤口愈合并发症的关联。此外,在FB的连续尺度上探讨并发症风险。
我们纳入了303例患者:44例属于低FB组,108例属于中FB组,151例属于高FB组。围手术期FB的中位数[四分位间距]分别为-0.9L[-1.4,-0.6]、0.9L[0.5,1.3]和3.8L[2.7,5.3]。高FB组发生心肺并发症的风险显著更高,为3.4(1.5-7.6),p=0.002(比值比(95%置信区间))。在液体平衡的连续尺度上,心肺并发症风险在-1L至1L时最小。
在胃肠道梗阻或穿孔急诊手术后,液体平衡<2.0L与降低心肺并发症风险相关,且不增加肾脏并发症。