Clarke Gerard Janez Brett, Follestad Turid, Skandsen Toril, Zetterberg Henrik, Vik Anne, Blennow Kaj, Olsen Alexander, Håberg Asta Kristine
Department of Radiology and Nuclear Medicine, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway.
Department of Neuromedicine and Movement Sciences, NTNU, Trondheim, Norway.
J Neuroinflammation. 2024 Apr 27;21(1):109. doi: 10.1186/s12974-024-03094-8.
Identifying individuals with intracranial injuries following mild traumatic brain injury (mTBI), i.e. complicated mTBI cases, is important for follow-up and prognostication. The main aims of our study were (1) to assess the temporal evolution of blood biomarkers of CNS injury and inflammation in individuals with complicated mTBI determined on computer tomography (CT) and magnetic resonance imaging (MRI); (2) to assess the corresponding discriminability of both single- and multi-biomarker panels, from acute to chronic phases after injury.
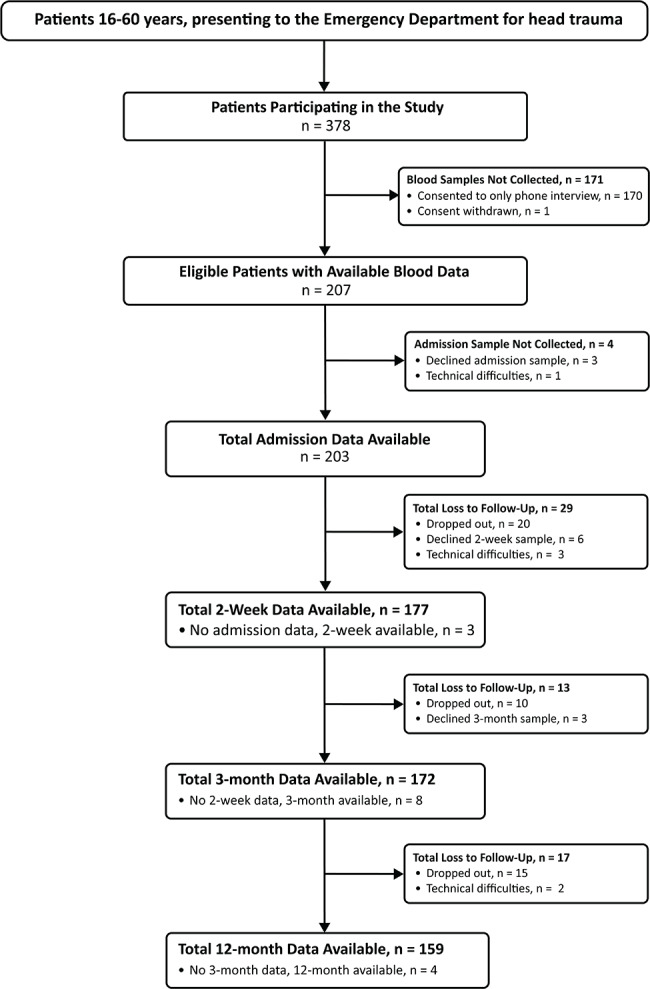
Patients with mTBI (n = 207), defined as Glasgow Coma Scale score between 13 and 15, loss of consciousness < 30 min and post-traumatic amnesia < 24 h, were included. Complicated mTBI - i.e., presence of any traumatic intracranial injury on neuroimaging - was present in 8% (n = 16) on CT (CT+) and 12% (n = 25) on MRI (MRI+). Blood biomarkers were sampled at four timepoints following injury: admission (within 72 h), 2 weeks (± 3 days), 3 months (± 2 weeks) and 12 months (± 1 month). CNS biomarkers included were glial fibrillary acidic protein (GFAP), neurofilament light (NFL) and tau, along with 12 inflammation markers.
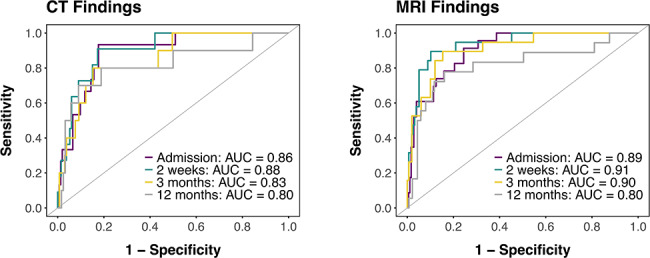
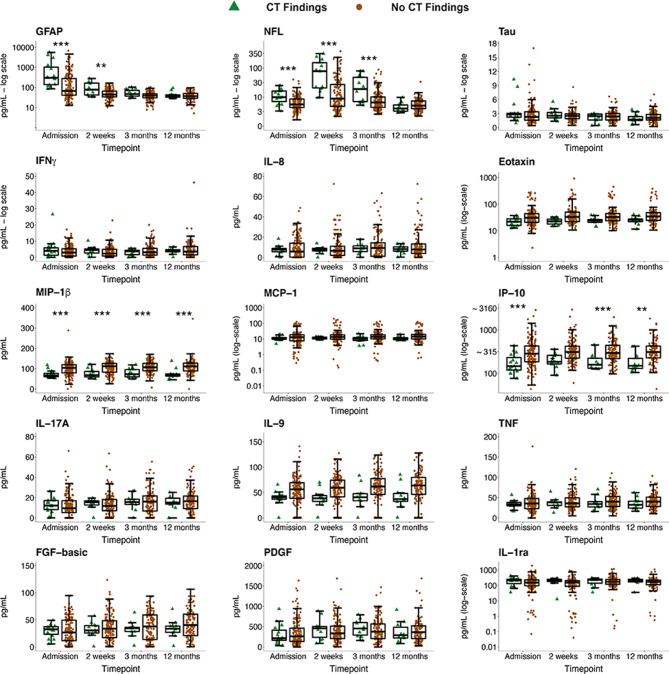
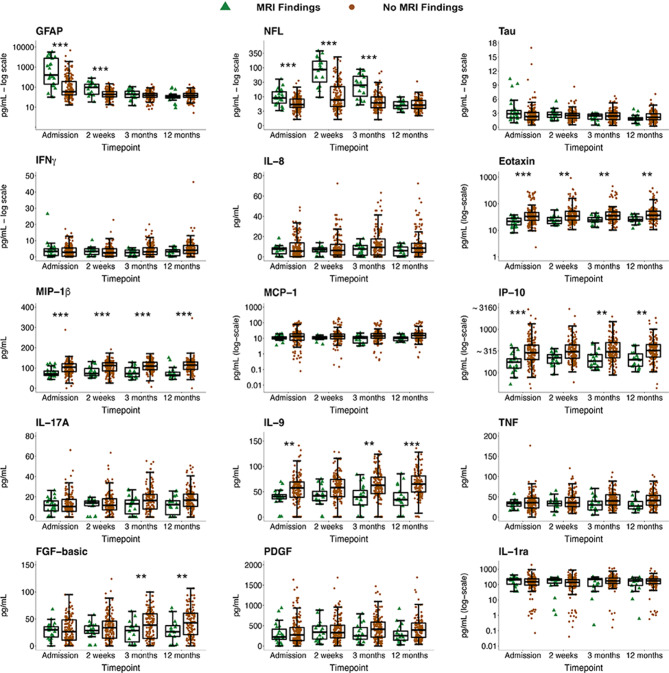
The most discriminative single biomarkers of traumatic intracranial injury were GFAP at admission (CT+: AUC = 0.78; MRI+: AUC = 0.82), and NFL at 2 weeks (CT+: AUC = 0.81; MRI+: AUC = 0.89) and 3 months (MRI+: AUC = 0.86). MIP-1β and IP-10 concentrations were significantly lower across follow-up period in individuals who were CT+ and MRI+. Eotaxin and IL-9 were significantly lower in individuals who were MRI+ only. FGF-basic concentrations increased over time in MRI- individuals and were significantly higher than MRI+ individuals at 3 and 12 months. Multi-biomarker panels improved discriminability over single biomarkers at all timepoints (AUCs > 0.85 for admission and 2-week models classifying CT+ and AUC ≈ 0.90 for admission, 2-week and 3-month models classifying MRI+).
The CNS biomarkers GFAP and NFL were useful single diagnostic biomarkers of complicated mTBI, especially in acute and subacute phases after mTBI. Several inflammation markers were suppressed in patients with complicated versus uncomplicated mTBI and remained so even after 12 months. Multi-biomarker panels improved diagnostic accuracy at all timepoints, though at acute and 2-week timepoints, the single biomarkers GFAP and NFL, respectively, displayed similar accuracy compared to multi-biomarker panels.
识别轻度创伤性脑损伤(mTBI)后发生颅内损伤的个体,即复杂性mTBI病例,对于随访和预后评估很重要。我们研究的主要目的是:(1)评估经计算机断层扫描(CT)和磁共振成像(MRI)确诊的复杂性mTBI个体中中枢神经系统(CNS)损伤和炎症血液生物标志物的时间演变;(2)评估从损伤后急性期到慢性期单生物标志物和多生物标志物组合的相应判别能力。
纳入mTBI患者(n = 207),定义为格拉斯哥昏迷量表评分为13至15分、意识丧失<30分钟且创伤后遗忘<24小时。CT检查显示8%(n = 16)存在复杂性mTBI,即神经影像学上有任何创伤性颅内损伤(CT+),MRI检查显示12%(n = 25)存在(MRI+)。在损伤后的四个时间点采集血液生物标志物:入院时(72小时内)、2周(±3天)、3个月(±2周)和12个月(±1个月)。纳入的CNS生物标志物包括胶质纤维酸性蛋白(GFAP)、神经丝轻链(NFL)和tau,以及12种炎症标志物。
创伤性颅内损伤最具判别力的单生物标志物是入院时的GFAP(CT+:AUC = 0.78;MRI+:AUC = 0.82),2周时的NFL(CT+:AUC = 0.81;MRI+:AUC = 0.89)和3个月时的NFL(MRI+:AUC = 0.86)。在CT+和MRI+个体的整个随访期间,MIP-1β和IP-10浓度显著降低。仅在MRI+个体中,嗜酸性粒细胞趋化因子和IL-9显著降低。碱性成纤维细胞生长因子(FGF-basic)浓度在MRI-个体中随时间增加,在3个月和12个月时显著高于MRI+个体。在所有时间点,多生物标志物组合比单生物标志物具有更好的判别能力(用于分类CT+的入院和2周模型的AUC>0.85,用于分类MRI+的入院、2周和3个月模型的AUC≈0.90)。
CNS生物标志物GFAP和NFL是复杂性mTBI有用的单诊断生物标志物,尤其是在mTBI后的急性期和亚急性期。与非复杂性mTBI患者相比,复杂性mTBI患者的几种炎症标志物受到抑制,并且在12个月后仍然如此。多生物标志物组合在所有时间点均提高了诊断准确性,不过在急性期和2周时间点,单生物标志物GFAP和NFL分别显示出与多生物标志物组合相似的准确性。