Research Department, Gillette Children's, St. Paul, MN, USA.
University of Minnesota Medical School, Minneapolis, MN, USA.
Spine Deform. 2024 Sep;12(5):1393-1401. doi: 10.1007/s43390-024-00878-z. Epub 2024 Apr 29.
To describe the incidence of reoperation and factors contributing to surgical revision within a minimum of 10 years after spinal fusion for scoliosis in patients with nonambulatory cerebral palsy (CP).
We conducted a retrospective review of consecutive nonambulatory patients with CP who underwent primary spinal fusion at a single specialty care center with a minimum of 10 years from their index surgery (surgery dates 2001-2011). Causes of reoperation were classified as implant failure/pseudoarthrosis, surgical site infection (SSI), proximal junctional kyphosis, prominent/symptomatic implants, and implant removal. Reoperation rates with 95% confidence intervals were calculated for each time interval, and an actuarial survival curve was generated.
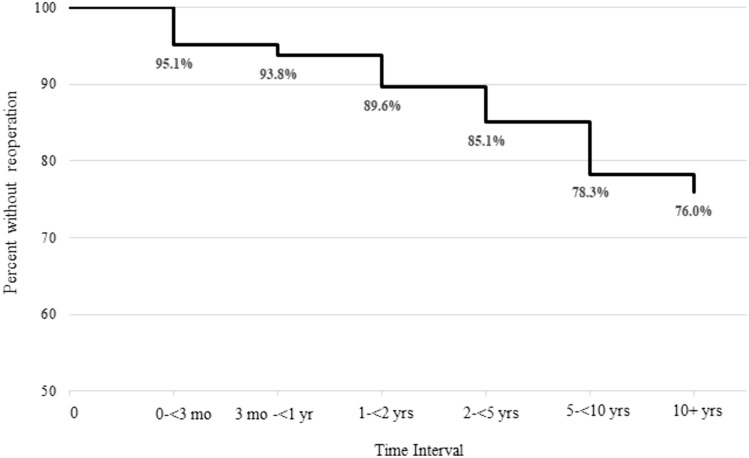
144 patients met inclusion criteria (mean age = 14.3 ± 2.6 years, 62.5% male); 85.4% had 5 years follow-up data; and 66.0% had 10 years follow-up data. Estimates from the actuarial analysis suggest that 14.9% (95% CI: 10.0-22.0) underwent reoperation by 5 years postsurgery, and 21.7% (95% CI: 15.4-30.1) underwent reoperation by 10 years postsurgery. The most common causes for reoperation were implant failure/pseudoarthrosis, SSI, and prominent/symptomatic implants.
To our knowledge, this study is the largest long-term follow-up of nonambulatory patients with CP and neuromuscular scoliosis who underwent spinal fusion. Approximately 22% of these patients required reoperation 10 years after their index surgery, primarily due to implant failure/pseudoarthrosis, SSI, and prominent/symptomatic implants. Complications and reoperations continued throughout the 10 years period after index surgery, reinforcing the need for long-term follow-up as these patients transition into adulthood.
III.
描述非瘫痪型脑瘫患者脊柱融合术后至少 10 年内再次手术的发生率和导致手术翻修的因素。
我们对在单一家专科中心接受初次脊柱融合术的连续非瘫痪型脑瘫患者进行了回顾性研究,这些患者的手术日期为 2001 年至 2011 年,其随访时间至少为 10 年。将再次手术的原因分为内植物失败/假关节、手术部位感染(SSI)、近端交界性后凸、突出/有症状的内植物和内植物取出。计算了每个时间间隔的再手术率和 95%置信区间,并生成了生存分析曲线。
144 名患者符合纳入标准(平均年龄 14.3±2.6 岁,62.5%为男性);85.4%的患者有 5 年随访数据;66.0%的患者有 10 年随访数据。生存分析估计,术后 5 年有 14.9%(95%CI:10.0-22.0)的患者需要再次手术,术后 10 年有 21.7%(95%CI:15.4-30.1)的患者需要再次手术。再次手术最常见的原因是内植物失败/假关节、SSI 和突出/有症状的内植物。
据我们所知,这是对接受脊柱融合术的非瘫痪型脑瘫伴神经肌肉性脊柱侧凸患者进行的最大规模的长期随访研究。这些患者中有 22%左右在初次手术后 10 年内需要再次手术,主要原因是内植物失败/假关节、SSI 和突出/有症状的内植物。并发症和再次手术在初次手术后的 10 年内持续发生,这强化了需要对这些患者进行长期随访的必要性,因为他们即将进入成年期。
III 级。