Hao Chenxiao, Hao Rui, Zhao Huiying, Zhang Yong, Sheng Ming, An Youzhong
Department of Critical Care Medicine, Peking University People's Hospital, Beijing, 100044, China.
School of Computer Science, Beijing University of Posts and Telecommunications, Haidian District, Beijing, 100876, China.
Heliyon. 2024 Mar 25;10(7):e28520. doi: 10.1016/j.heliyon.2024.e28520. eCollection 2024 Apr 15.
The recognition of sepsis as a heterogeneous syndrome necessitates identifying distinct subphenotypes to select targeted treatment.
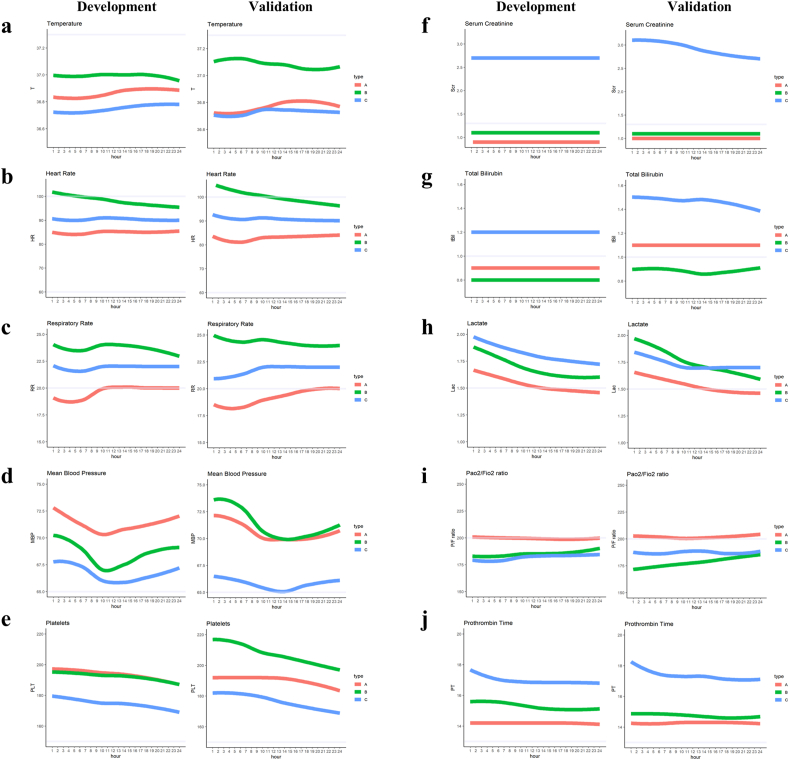
Patients with sepsis from the MIMIC-IV database (2008-2019) were randomly divided into a development cohort (80%) and an internal validation cohort (20%). Patients with sepsis from the ICU database of Peking University People's Hospital (2008-2022) were included in the external validation cohort. Time-series k-means clustering analysis and dynamic time warping was performed to develop and validate sepsis subphenotypes by analyzing the trends of 21 vital signs and laboratory indicators within 24 h after sepsis onset. Inflammatory biomarkers were compared in the ICU database of Peking University People's Hospital, whereas treatment heterogeneity was compared in the MIMIC-IV database.
Three sub-phenotypes were identified in the development cohort. Type A patients (N = 2525, 47%) exhibited stable vital signs and fair organ function, type B (N = 1552, 29%) was exhibited an obvious inflammatory response and stable organ function, and type C (N = 1251, 24%) exhibited severely impaired organ function with a deteriorating tendency. Type C demonstrated the highest mortality rate (33%) and levels of inflammatory biomarkers, followed by type B (24%), whereas type A exhibited the lowest mortality rate (11%) and levels of inflammatory biomarkers. These subphenotypes were confirmed in both the internal and external cohorts, demonstrating similar features and comparable mortality rates. In type C patients, survivors had significantly lower fluid intake within 24 h after sepsis onset (median 2891 mL, interquartile range (IQR) 1530-5470 mL) than that in non-survivors (median 4342 mL, IQR 2189-7305 mL). For types B and C, survivors showed a higher proportion of indwelling central venous catheters (p < 0.05).
Three novel phenotypes of patients with sepsis were identified and validated using time-series data, revealing significant heterogeneity in inflammatory biomarkers, treatments, and consistency across cohorts.
鉴于脓毒症是一种异质性综合征,有必要识别出不同的亚表型以选择针对性治疗。
将来自多中心重症医学信息库第四版(MIMIC-IV,2008 - 2019年)的脓毒症患者随机分为一个开发队列(80%)和一个内部验证队列(20%)。来自北京大学人民医院重症监护病房数据库(2008 - 2022年)的脓毒症患者被纳入外部验证队列。通过分析脓毒症发作后24小时内21项生命体征和实验室指标的趋势,进行时间序列k均值聚类分析和动态时间规整,以开发和验证脓毒症亚表型。在北京大学人民医院重症监护病房数据库中比较炎症生物标志物,而在MIMIC-IV数据库中比较治疗异质性。
在开发队列中识别出三种亚表型。A型患者(N = 2525,47%)生命体征稳定,器官功能尚可;B型(N = 1552,29%)表现出明显的炎症反应且器官功能稳定;C型(N = 1251,24%)器官功能严重受损且有恶化趋势。C型患者的死亡率(33%)和炎症生物标志物水平最高,其次是B型(24%),而A型患者的死亡率(11%)和炎症生物标志物水平最低。这些亚表型在内部和外部队列中均得到证实,显示出相似的特征和相当的死亡率。在C型患者中,幸存者在脓毒症发作后24小时内的液体摄入量(中位数2891毫升,四分位间距(IQR)1530 - 5470毫升)显著低于非幸存者(中位数4342毫升,IQR 2189 - 7305毫升)。对于B型和C型患者,幸存者中留置中心静脉导管的比例更高(p < 0.05)。
利用时间序列数据识别并验证了三种新型脓毒症患者表型,揭示了炎症生物标志物、治疗方面的显著异质性以及各队列间的一致性。