Yale School of Medicine, New Haven, Connecticut, USA.
The University of Texas at Austin, Austin, Texas, USA.
J Clin Invest. 2024 May 1;134(9):e176640. doi: 10.1172/JCI176640.
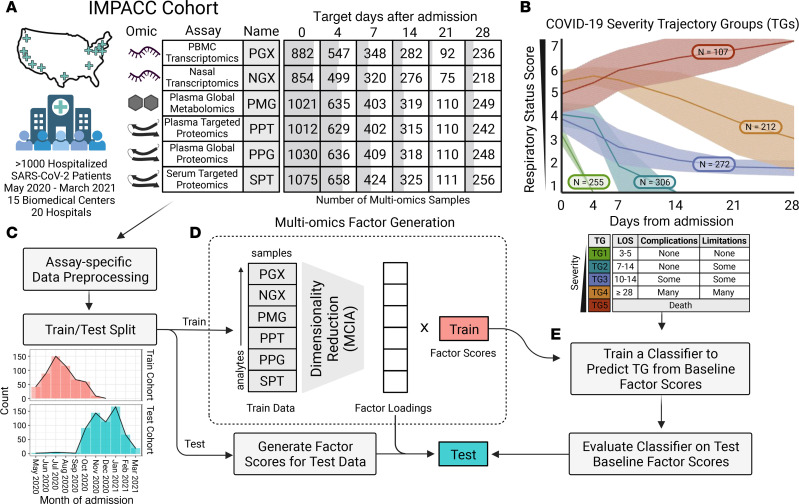
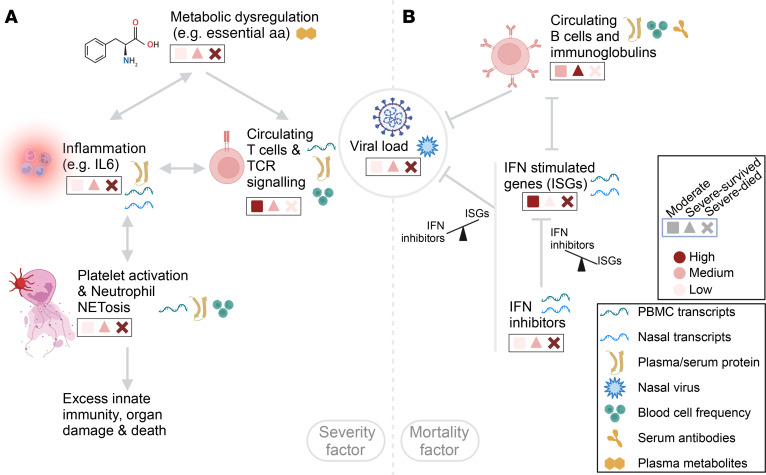
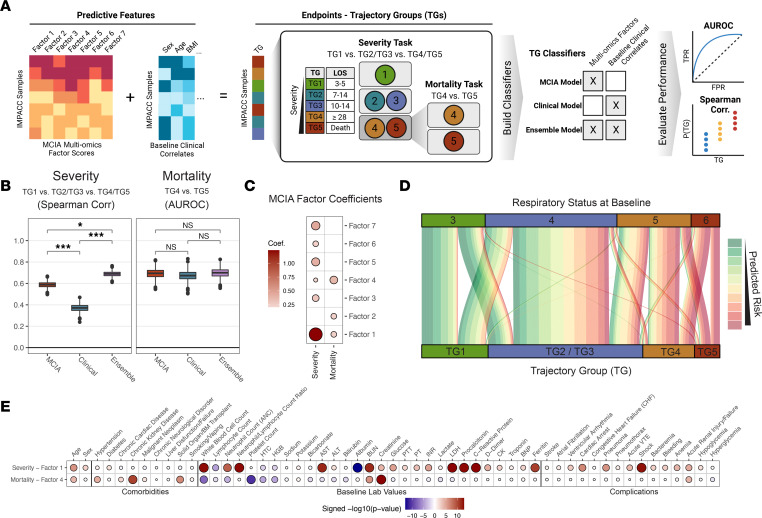
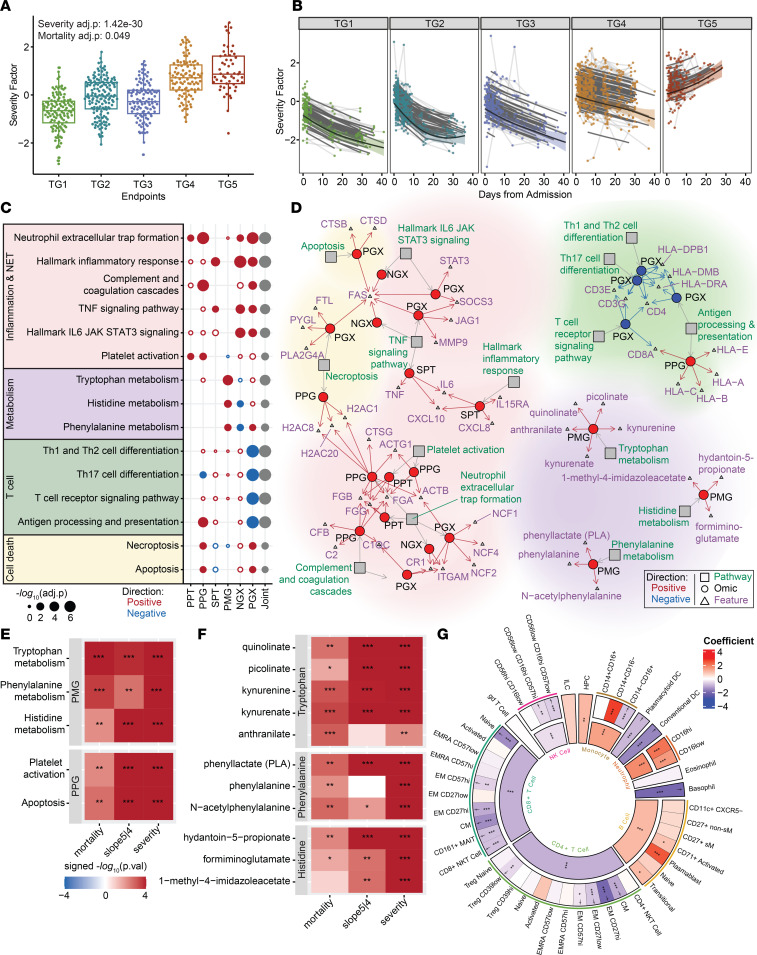
BACKGROUNDPatients hospitalized for COVID-19 exhibit diverse clinical outcomes, with outcomes for some individuals diverging over time even though their initial disease severity appears similar to that of other patients. A systematic evaluation of molecular and cellular profiles over the full disease course can link immune programs and their coordination with progression heterogeneity.METHODSWe performed deep immunophenotyping and conducted longitudinal multiomics modeling, integrating 10 assays for 1,152 Immunophenotyping Assessment in a COVID-19 Cohort (IMPACC) study participants and identifying several immune cascades that were significant drivers of differential clinical outcomes.RESULTSIncreasing disease severity was driven by a temporal pattern that began with the early upregulation of immunosuppressive metabolites and then elevated levels of inflammatory cytokines, signatures of coagulation, formation of neutrophil extracellular traps, and T cell functional dysregulation. A second immune cascade, predictive of 28-day mortality among critically ill patients, was characterized by reduced total plasma Igs and B cells and dysregulated IFN responsiveness. We demonstrated that the balance disruption between IFN-stimulated genes and IFN inhibitors is a crucial biomarker of COVID-19 mortality, potentially contributing to failure of viral clearance in patients with fatal illness.CONCLUSIONOur longitudinal multiomics profiling study revealed temporal coordination across diverse omics that potentially explain the disease progression, providing insights that can inform the targeted development of therapies for patients hospitalized with COVID-19, especially those who are critically ill.TRIAL REGISTRATIONClinicalTrials.gov NCT04378777.FUNDINGNIH (5R01AI135803-03, 5U19AI118608-04, 5U19AI128910-04, 4U19AI090023-11, 4U19AI118610-06, R01AI145835-01A1S1, 5U19AI062629-17, 5U19AI057229-17, 5U19AI125357-05, 5U19AI128913-03, 3U19AI077439-13, 5U54AI142766-03, 5R01AI104870-07, 3U19AI089992-09, 3U19AI128913-03, and 5T32DA018926-18); NIAID, NIH (3U19AI1289130, U19AI128913-04S1, and R01AI122220); and National Science Foundation (DMS2310836).
因 COVID-19 住院的患者表现出不同的临床结局,尽管他们最初的疾病严重程度与其他患者相似,但一些患者的病情随时间推移而出现差异。对整个疾病过程中的分子和细胞特征进行系统评估可以将免疫程序及其与进展异质性的协调联系起来。
我们进行了深度免疫表型分析,并进行了纵向多组学建模,对 10 项免疫表型评估测试对 1152 名 COVID-19 队列研究(IMPACC)参与者进行了整合,并确定了几个对差异临床结局具有重要驱动作用的免疫级联反应。
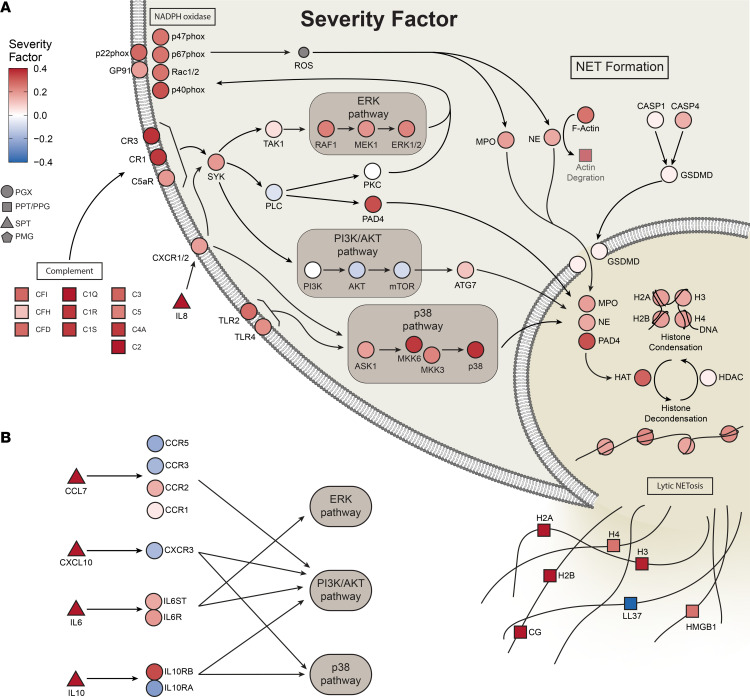
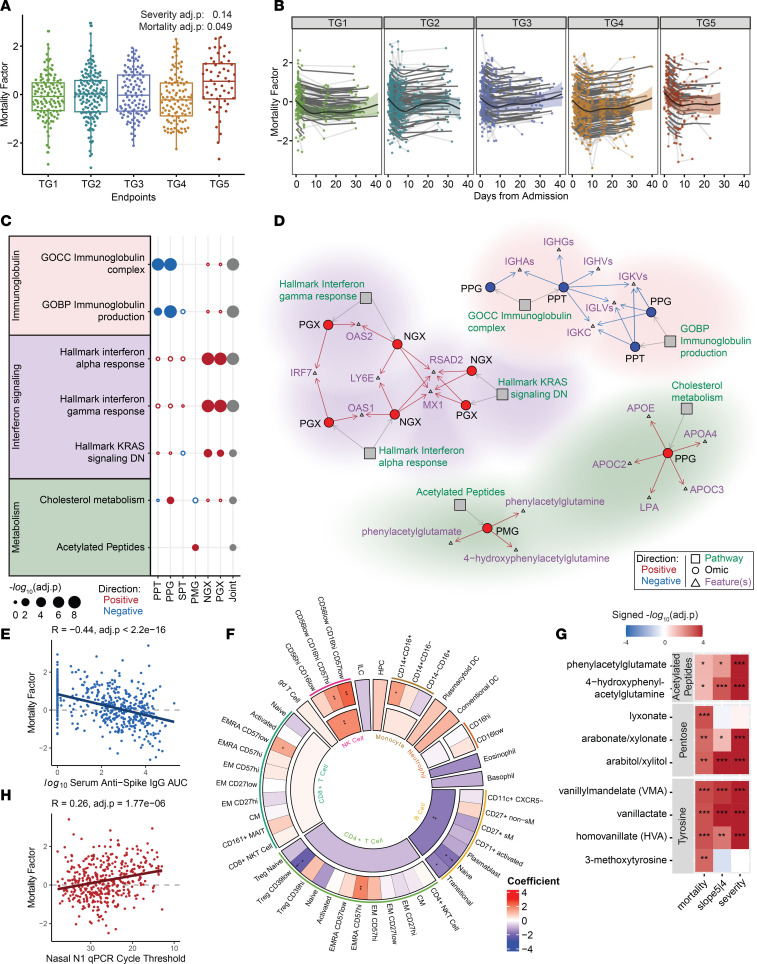
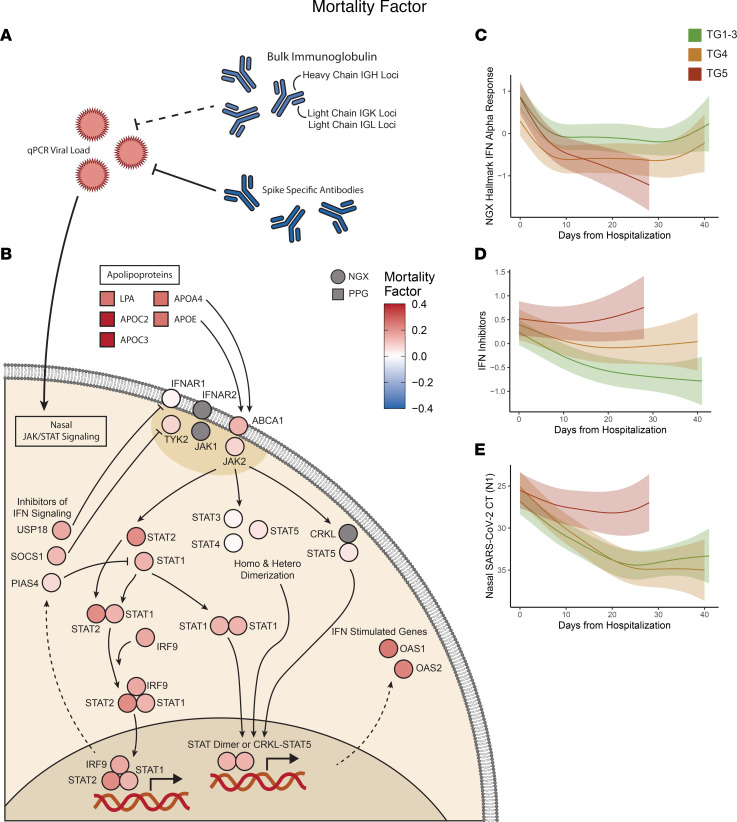
疾病严重程度的增加是由一个时间模式驱动的,该模式始于早期上调免疫抑制代谢物,然后是炎症细胞因子水平升高、凝血特征、中性粒细胞细胞外陷阱的形成和 T 细胞功能失调。第二个预测危重症患者 28 天死亡率的免疫级联反应的特征是总血浆 Ig 和 B 细胞减少以及 IFN 反应失调。我们证明,IFN 刺激基因和 IFN 抑制剂之间的平衡破坏是 COVID-19 死亡率的一个关键生物标志物,可能导致致命疾病患者的病毒清除失败。
我们的纵向多组学分析研究揭示了不同组学之间的时间协调,这可能解释了疾病的进展,为 COVID-19 住院患者,特别是危重症患者的靶向治疗开发提供了见解。
ClinicalTrials.gov NCT04378777。
NIH(5R01AI135803-03、5U19AI118608-04、5U19AI128910-04、4U19AI090023-11、4U19AI118610-06、R01AI145835-01A1S1、5U19AI062629-17、5U19AI057229-17、5U19AI125357-05、5U19AI128913-03、3U19AI077439-13、5U54AI142766-03、5R01AI104870-07、3U19AI089992-09、3U19AI128913-03、5T32DA018926-18);NIAID,NIH(3U19AI1289130、U19AI128913-04S1 和 R01AI122220);以及美国国家科学基金会(DMS2310836)。