Kawai Taketo, Matsuyama Hideyasu, Kobayashi Keita, Ikeda Atsushi, Miyake Makito, Nishimoto Koshiro, Matsushita Yuto, Nishiyama Hiroyuki, Fujimoto Kiyohide, Oyama Masafumi, Miyake Hideaki, Azuma Haruhito, Inoue Keiji, Mitsui Takahiko, Kawakita Mutsushi, Oyama Chikara, Mizokami Atsushi, Abe Takashige, Kuroiwa Hajime, Kume Haruki
Department of Urology, Teikyo University School of Medicine, Tokyo, Japan.
Department of Urology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Int J Urol. 2024 Aug;31(8):906-912. doi: 10.1111/iju.15483. Epub 2024 May 2.
In a primary analysis of data from the BRIGHT study (UMIN000035712), photodynamic diagnosis-assisted transurethral resection of bladder tumor (PDD-TURBT) using oral 5-aminolevulinic acid hydrochloride reduced residual tumors in high-risk non-muscle invasive bladder cancer (NMIBC). We aimed to evaluate the effectiveness of PDD-TURBT for intravesical recurrence after a second transurethral resection for high-risk NMIBC.
High-risk NMIBC patients initially treated with PDD-TURBT (PDD group) were prospectively registered between 2018 and 2020. High-risk patients with NMIBC who were initially treated with white-light TURBT (WL group) were retrospectively registered. Intravesical recurrence-free survival after the second transurethral resection was compared between the PDD and WL groups using propensity score matching analysis.
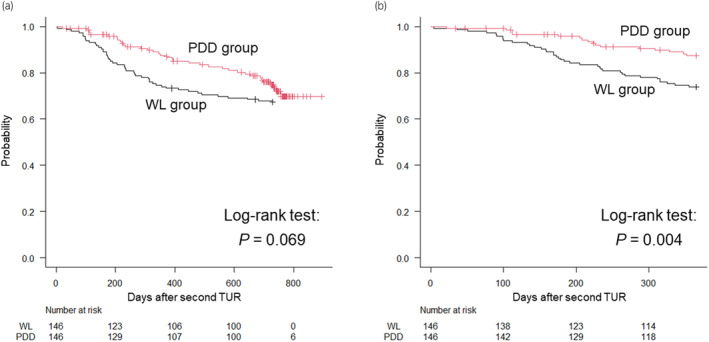
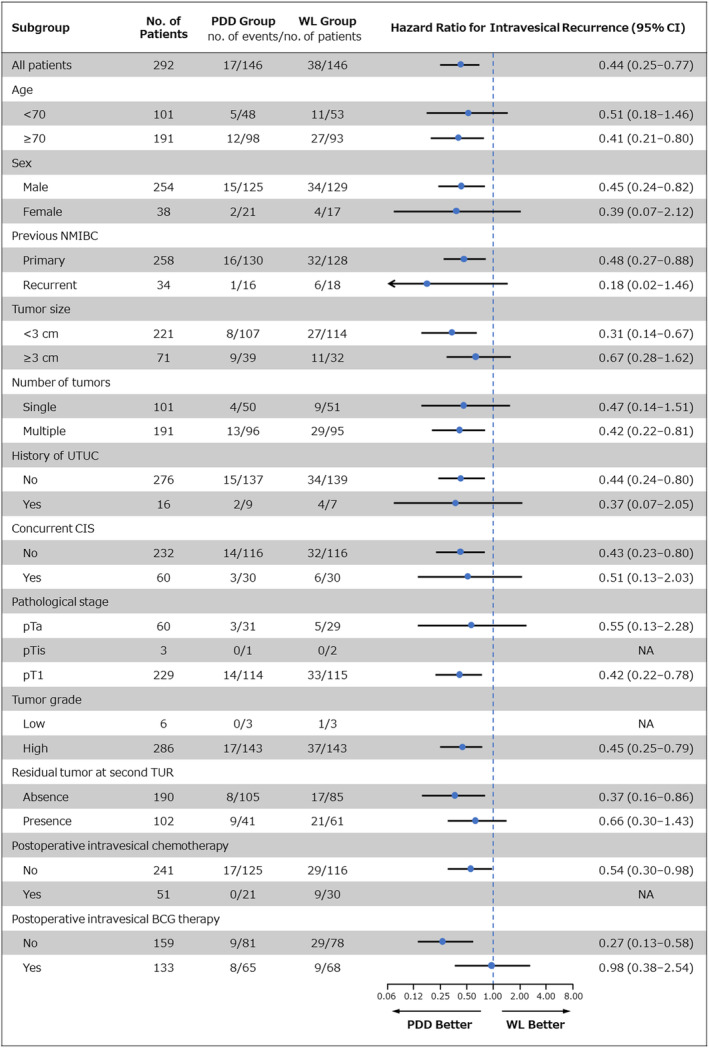
In total, 177 patients were enrolled in the PDD group, and 306 patients were registered in the WL group. After propensity score matching (146 cases in each group), intravesical recurrence within 1 year was significantly less frequent in the PDD group than in the WL group (p = 0.004; hazard ratio [HR] 0.44, 95% confidence interval [CI]: 0.25-0.77). In subgroup analysis, PDD-TURBT showed a particularly high efficacy in reducing intravesical recurrence within 1 year, especially in cases of tumors measuring less than 3 cm (p = 0.003; HR 0.31, 95% CI: 0.14-0.67), absence of residual tumor at second transurethral resection (p = 0.020; HR 0.37, 95% CI: 0.16-0.86), and no postoperative intravesical Bacillus Calmette-Guérin therapy (p < 0.001; HR 0.27, 95% CI: 0.13-0.58).
PDD-TURBT may reduce short-term intravesical recurrence in patients with high-risk NMIBC.
在对BRIGHT研究(UMIN000035712)的数据进行的初步分析中,使用口服盐酸5-氨基酮戊酸的光动力诊断辅助经尿道膀胱肿瘤切除术(PDD-TURBT)可减少高危非肌层浸润性膀胱癌(NMIBC)的残留肿瘤。我们旨在评估PDD-TURBT对高危NMIBC二次经尿道切除术后膀胱内复发的有效性。
2018年至2020年期间前瞻性登记了最初接受PDD-TURBT治疗的高危NMIBC患者(PDD组)。对最初接受白光TURBT治疗的高危NMIBC患者进行回顾性登记。使用倾向评分匹配分析比较PDD组和WL组二次经尿道切除术后膀胱内无复发生存率。
PDD组共纳入177例患者,WL组登记了306例患者。倾向评分匹配后(每组146例),PDD组1年内膀胱内复发的频率明显低于WL组(p = 0.004;风险比[HR] 0.44,95%置信区间[CI]:0.25 - 0.77)。在亚组分析中,PDD-TURBT在减少1年内膀胱内复发方面显示出特别高的疗效,尤其是在肿瘤直径小于3 cm的病例中(p = 0.003;HR 0.31,95% CI:0.14 - 0.67)、二次经尿道切除术后无残留肿瘤的病例中(p = 0.020;HR 0.37,95% CI:0.16 - 0.86)以及未进行术后膀胱内卡介苗治疗的病例中(p < 0.001;HR 0.27,95% CI:0.13 - 0.58)。
PDD-TURBT可能降低高危NMIBC患者的短期膀胱内复发率。