Saied Zakaria, Zouari Rania, Rachdi Amine, Nabli Fatma, Ben Mohamed Dina, Ben Sassi Samia
National Institute Mongi Ben Hamida of Neurology of Tunis, Faculty of Medicine of Tunis, Tunis El Manar University, Tunisia.
National Institute Mongi Ben Hamida of Neurology of Tunis, Tunisia.
Heliyon. 2024 Apr 22;10(9):e30004. doi: 10.1016/j.heliyon.2024.e30004. eCollection 2024 May 15.
Primary Sjogren's syndrome (pSS) is an autoimmune exocrinopathy in which extraglandular signs of pSS are determinant for the prognosis. Involvement of both peripheral and central nervous system (CNS) are known to be among the sites of high systemic activity in pSS.
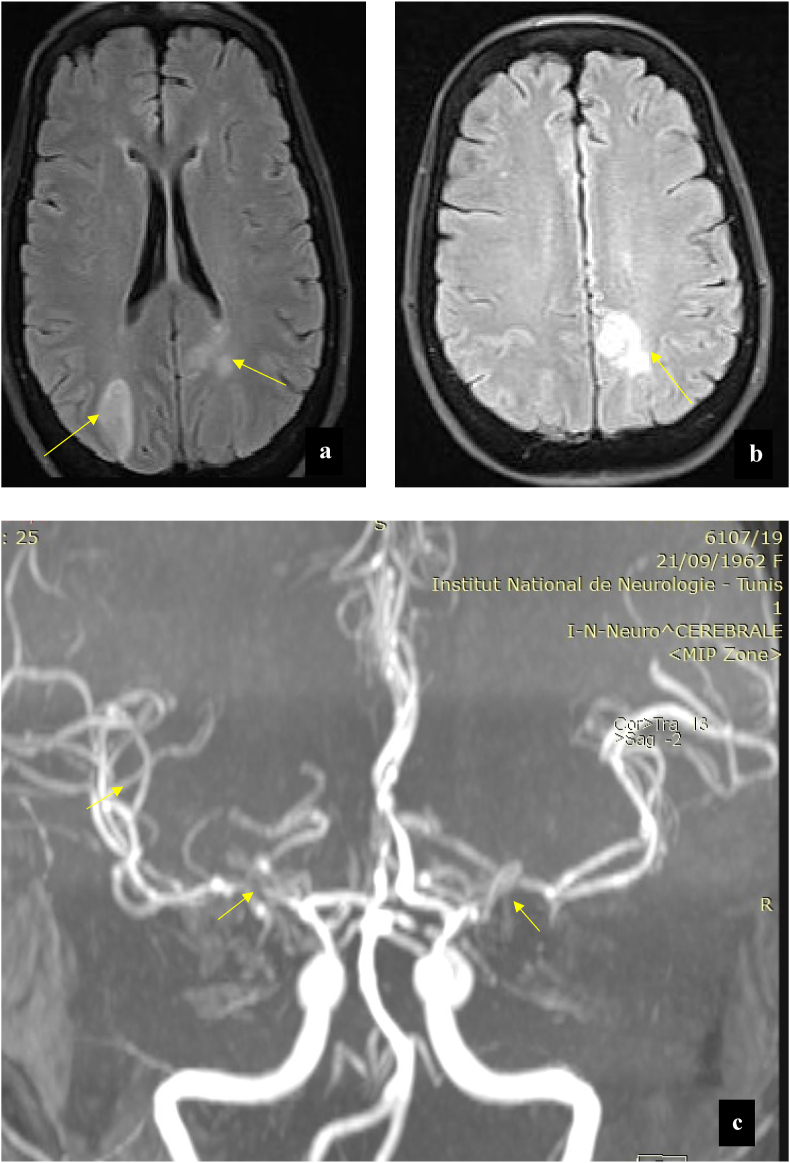
We, herein, report a case of a 57-year-old female patient with pSS presenting with typical (GBS), shortly followed by acute headaches accompanied by cortical blindness. Cerebral magnetic resonance imaging (MRI) demonstrated T2 signal abnormalities on the occipital region with narrowing and irregularities of the cerebral arteries, suggestive of CNS vasculitis.Subtle sicca symptoms occurring prior to neurological symptoms by 8 months together with immunological disturbances (anti-SSA, anti-SSB antibodies positivity, type II cryoglobulins positivity, and C4 hypocomplementemia) allowed us to retain the diagnosis of pSS. Recovery of motor symptoms was possible under the combined use of immunoglobulins and corticotherapy during the initial phase. A three-years follow-up confirmed progressive motor recovery and stabilization under 6-months cyclophosphamide cycles relayed by azathioprine therapy.
Neurological complications can be inaugural in lead to urgent investigations and treatment. Peripheral and central neurological manifestations can coexist. The approach should integrate careful clinical assessment, as well as radiological and immunological findings.
原发性干燥综合征(pSS)是一种自身免疫性外分泌病,其中pSS的腺外表现对预后起决定性作用。已知外周和中枢神经系统(CNS)受累是pSS全身高活动部位之一。
在此,我们报告一例57岁女性pSS患者,该患者出现典型的吉兰-巴雷综合征(GBS),随后不久出现急性头痛并伴有皮质盲。脑磁共振成像(MRI)显示枕叶区域T2信号异常,脑动脉变窄且不规则,提示中枢神经系统血管炎。神经症状出现前8个月出现的轻微干燥症状以及免疫紊乱(抗SSA、抗SSB抗体阳性、II型冷球蛋白阳性和C4低补体血症)使我们得以确诊pSS。在初始阶段联合使用免疫球蛋白和皮质类固醇治疗后,运动症状有可能恢复。三年随访证实,在硫唑嘌呤治疗接力的6个月环磷酰胺周期下,运动功能逐渐恢复并稳定。
神经并发症可能首发,导致紧急检查和治疗。外周和中枢神经表现可能同时存在。治疗方法应综合仔细的临床评估以及影像学和免疫学检查结果。