Departmento de Ingeniería Mecánica y Fabricación, Universidad de Sevilla, 41092, Seville, Spain.
School of Mechanical, Medical and Process Engineering, Queensland University of Technology, Brisbane, QLD, 4000, Australia.
Biomech Model Mechanobiol. 2024 Aug;23(4):1393-1409. doi: 10.1007/s10237-024-01846-2. Epub 2024 May 3.
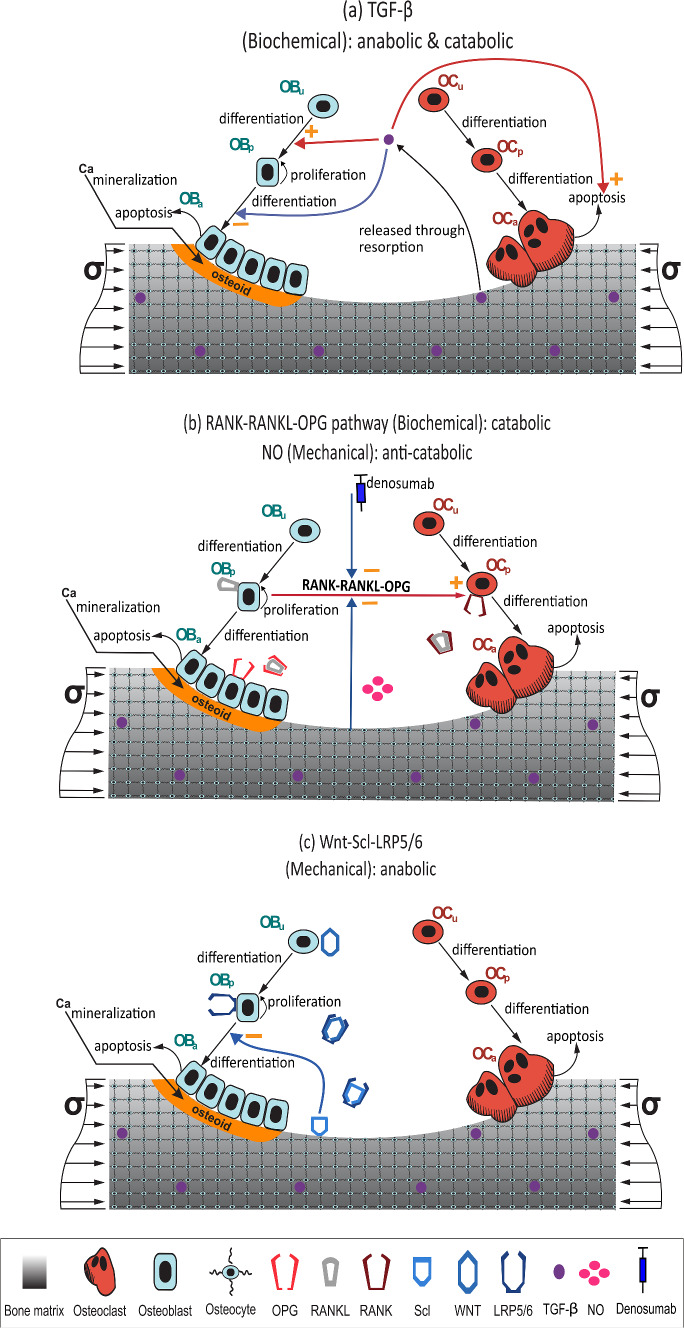
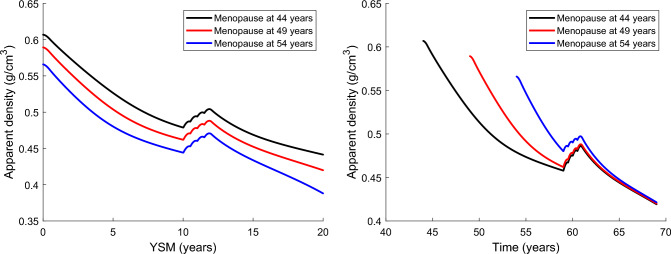
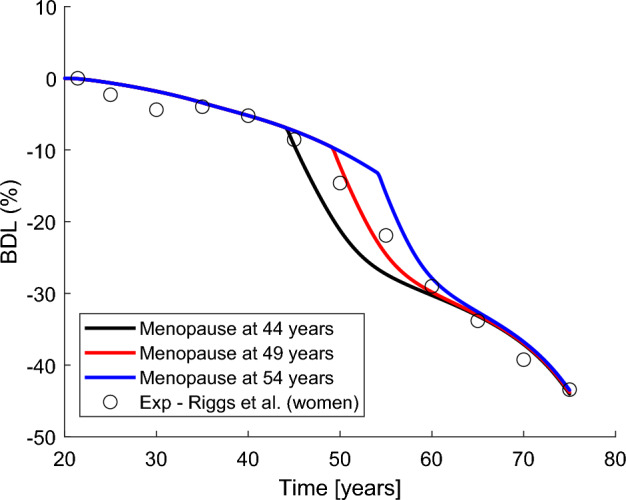
Numerical models of bone remodelling have traditionally been used to perform in silico tests of bone loss in postmenopausal women and also to simulate the response to different drug treatments. These models simulate the menopausal oestrogen decline by altering certain signalling pathways. However, they do not consider the simultaneous effect that ageing can have on cell function and bone remodelling, and thus on bone loss. Considering ageing and oestrogen decline together is important for designing osteoporosis treatments that can selectively counteract one or the other disease mechanism. A previously developed bone cell population model was adapted to consider the effect of ageing through: (1) the decrease of TGF- contained in the bone matrix and (2) an increased production of sclerostin by non-skeletal cells. Oestrogen deficiency is simulated in three different ways: (a) an increase in RANKL expression, (b) a decrease in OPG production, and (c) an increase in the responsiveness of osteoclasts to RANKL. The effect of ageing was validated using the cross-sectional study of (Riggs et al. in J Bone Miner Res 19: 1945-1954, 2004) on BMD of trabecular bone of the vertebral body of men. The joint effect of ageing and oestrogen deficiency was validated using these same clinical results but in women. In ageing, the effect of the increasing production of sclerostin is more important than the decrease of TGF- , while the three mechanisms used to simulate the effect of oestrogen deficiency produce almost identical responses. The results show that an early menopause leads to a lower average density in the fifth decade, but after the sixth decade the average density is independent of the age at menopause. Treatment of osteoporosis with denosumab was also simulated to conclude that the drug is not very effective if started before 10 years after menopause or before age 60.
骨重建的数值模型传统上被用于对绝经后妇女的骨丢失进行计算机模拟测试,也用于模拟不同药物治疗的反应。这些模型通过改变某些信号通路来模拟绝经后雌激素的下降。然而,它们没有考虑到衰老对细胞功能和骨重建的同时影响,以及由此对骨丢失的影响。考虑到衰老和雌激素下降的共同作用,对于设计可以选择性地对抗一种或另一种疾病机制的骨质疏松症治疗方法非常重要。之前开发的骨细胞群体模型通过以下两种方式进行了改编,以考虑衰老的影响:(1)减少骨基质中包含的 TGF-β;(2)非骨骼细胞中骨硬化素的产生增加。通过三种不同的方式模拟雌激素缺乏:(a)增加 RANKL 的表达,(b)减少 OPG 的产生,以及(c)增加破骨细胞对 RANKL 的反应性。使用(Riggs 等人在 J Bone Miner Res 19: 1945-1954, 2004 年)对男性椎体小梁骨骨密度的横断面研究验证了衰老的影响。使用这些相同的临床结果,但在女性中,验证了衰老和雌激素缺乏的联合影响。在衰老中,增加骨硬化素产生的影响比 TGF-β减少更为重要,而用于模拟雌激素缺乏影响的三种机制产生几乎相同的反应。结果表明,早期绝经导致第五个十年的平均密度降低,但在第六个十年后,平均密度与绝经年龄无关。还模拟了使用 denosumab 治疗骨质疏松症的情况,以得出结论,如果在绝经后 10 年或 60 岁之前开始治疗,该药物的效果不是很好。