Pneumology Service, Lucus Augusti University Hospital, EOXI Lugo, Monforte, Cervo, Spain.
Observational and Pragmatic Research Institute, Singapore, Singapore.
Am J Respir Crit Care Med. 2024 Oct 1;210(7):869-880. doi: 10.1164/rccm.202311-2192OC.
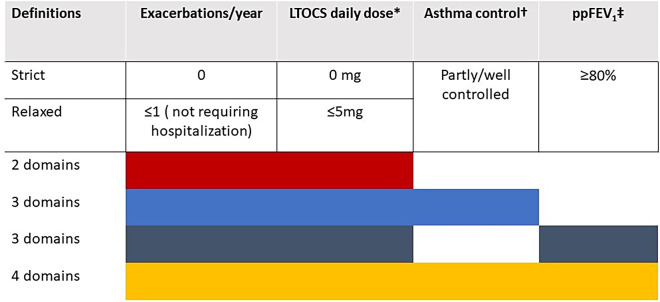
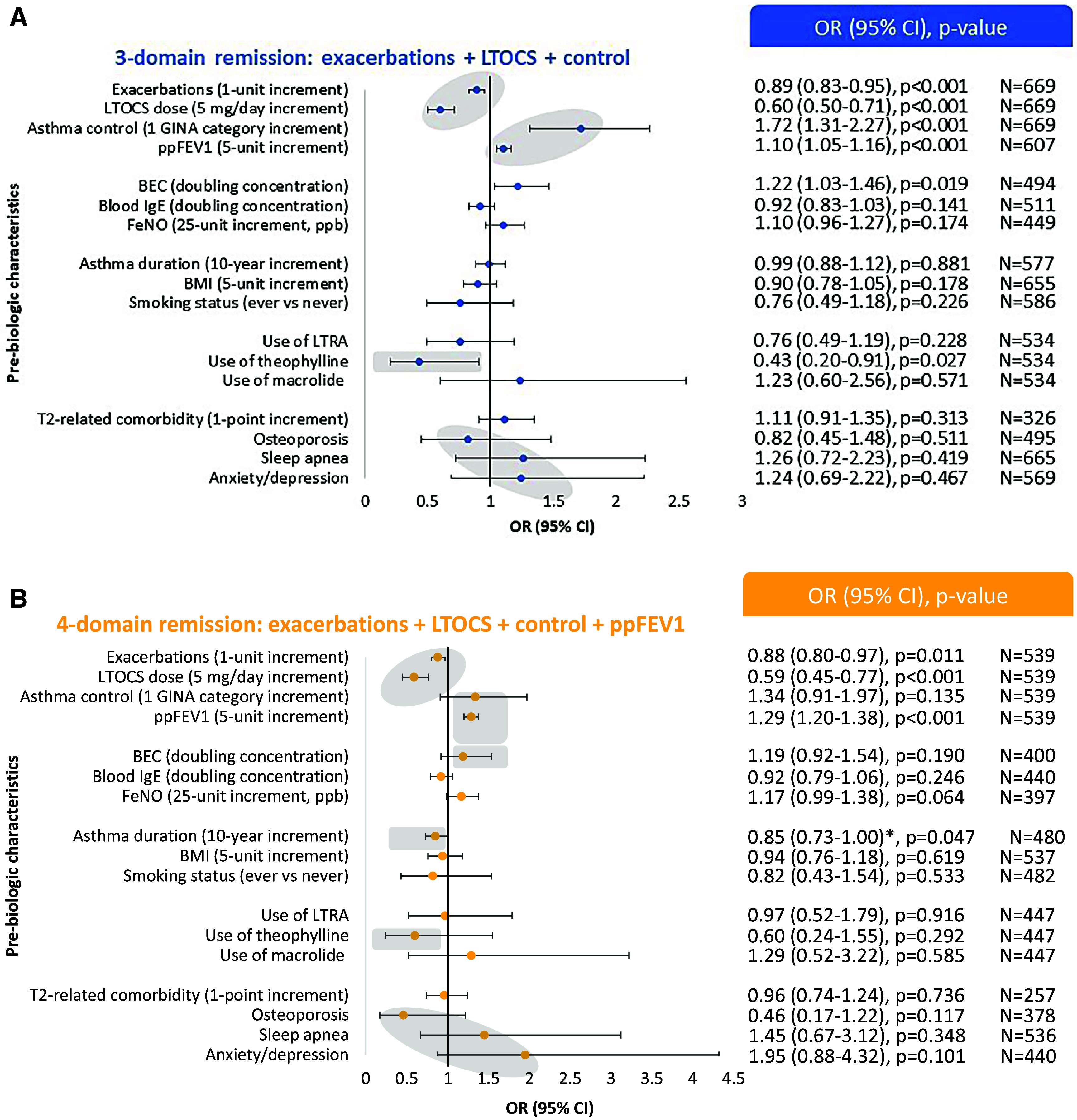
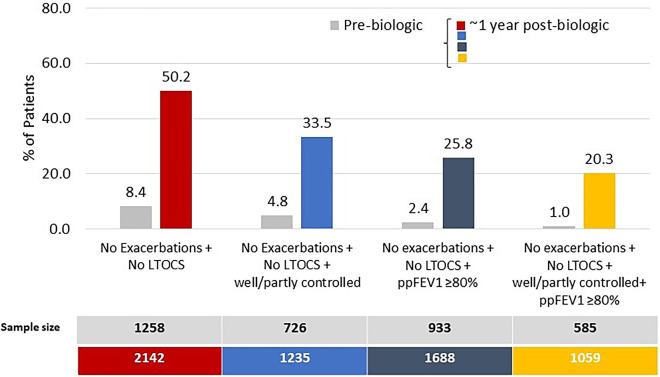
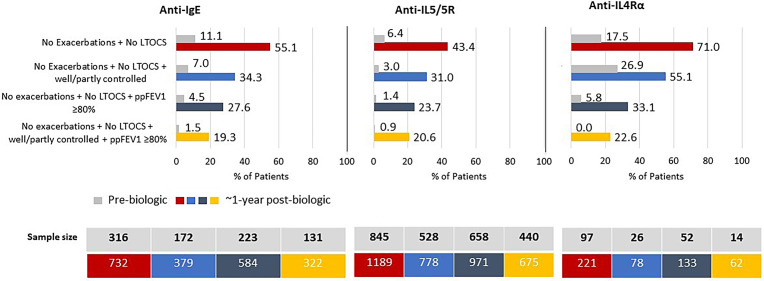
There is no consensus on criteria to include in an asthma remission definition in real life. Factors associated with achieving remission after biologic initiation remain poorly understood. To quantify the proportion of adults with severe asthma achieving multidomain-defined remission after biologic initiation and identify prebiologic characteristics associated with achieving remission that may be used to predict it. This was a longitudinal cohort study using data from 23 countries from the International Severe Asthma Registry. Four asthma outcome domains were assessed in the 1 year before and after biologic initiation. defined remission cutoffs were: 0 exacerbations/yr, no long-term oral corticosteroid (LTOCS), partly/well-controlled asthma, and percent predicted FEV ⩾ 80%. Remission was defined using two (exacerbations + LTOCS), three (+control or +lung function), and four of these domains. The association between prebiologic characteristics and postbiologic remission was assessed by multivariable analysis. A total of 50.2%, 33.5%, 25.8%, and 20.3% of patients met criteria for two-, three- (+control), three- (+lung function), and four-domain remission, respectively. The odds of achieving four-domain remission decreased by 15% for every additional 10 years of asthma duration (odds ratio, 0.85; 95% confidence interval, 0.73-1.00). The odds of remission increased in those with fewer exacerbations per year, lower LTOCS daily dose, better control, and better lung function before biologic initiation. One in five patients achieved four-domain remission within 1 year of biologic initiation. Patients with less severe impairment and shorter asthma duration at initiation had a greater chance of achieving remission after biologic treatment, indicating that biologic treatment should not be delayed if remission is the goal.
在现实生活中,对于纳入哮喘缓解定义的标准尚未达成共识。对于生物制剂治疗后实现缓解的相关因素仍知之甚少。本研究旨在定量评估生物制剂治疗后重度哮喘患者达到多维度定义缓解的比例,并识别与缓解相关的生物学前特征,这些特征可能有助于预测缓解。这是一项使用来自国际重度哮喘注册研究(International Severe Asthma Registry)的 23 个国家数据的纵向队列研究。在生物制剂治疗前和治疗后 1 年评估了 4 个哮喘结局领域。缓解的定义使用了以下 2 个(加重事件+口服激素)、3 个(+控制或+肺功能)和 4 个领域的缓解标准。通过多变量分析评估了生物学前特征与生物制剂治疗后缓解之间的关系。分别有 50.2%、33.5%、25.8%和 20.3%的患者符合 2 个、3 个(+控制)、3 个(+肺功能)和 4 个领域缓解标准。与实现 4 个领域缓解相比,哮喘病程每增加 10 年,达到 4 个领域缓解的可能性降低 15%(比值比,0.85;95%置信区间,0.73-1.00)。每年加重次数更少、口服激素日剂量更低、控制更好和肺功能更好的患者缓解可能性更高。有 1/5 的患者在开始生物制剂治疗后 1 年内达到了 4 个领域的缓解。在开始生物治疗时,病情较轻且哮喘病程较短的患者在生物治疗后缓解的机会更大,这表明如果缓解是目标,则不应延迟生物治疗。