Kato Naoki, Ishibashi Toshihiro, Otani Katharina, Abe Yukiko, Sano Tohru, Nagayama Gota, Fuga Michiyasu, Hataoka Shunsuke, Kan Issei, Murayama Yuichi
Department of Neurosurgery, The Jikei University School of Medicine Tokyo, Tokyo, Japan.
Siemens Healthcare K.K., Tokyo, Japan.
World Neurosurg X. 2024 Apr 21;23:100381. doi: 10.1016/j.wnsx.2024.100381. eCollection 2024 Jul.
To investigate on three-dimensional (3D) fusion images the apposition of low-profile visualized intraluminal support (LVIS) stents in intracranial aneurysms after treatment and assess inter-rater reliability.
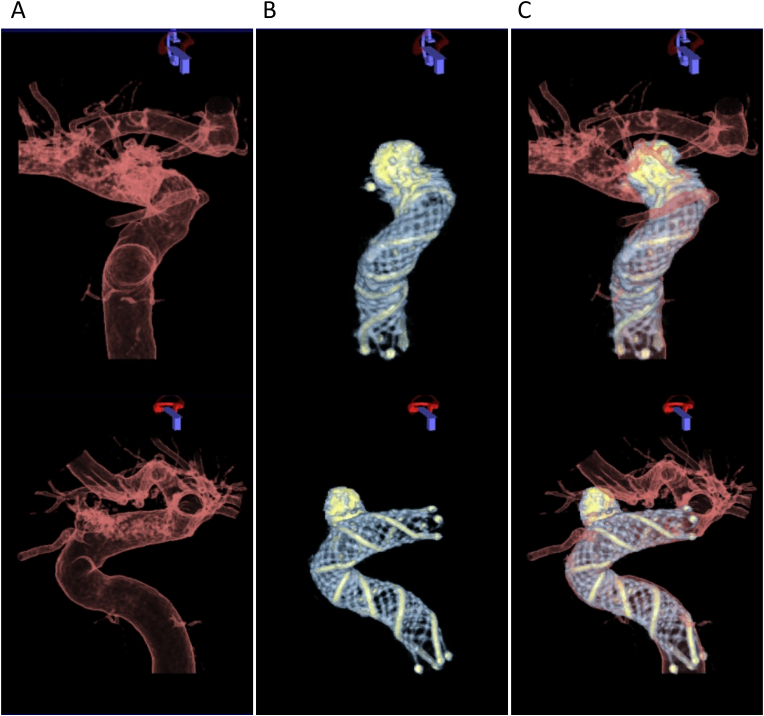
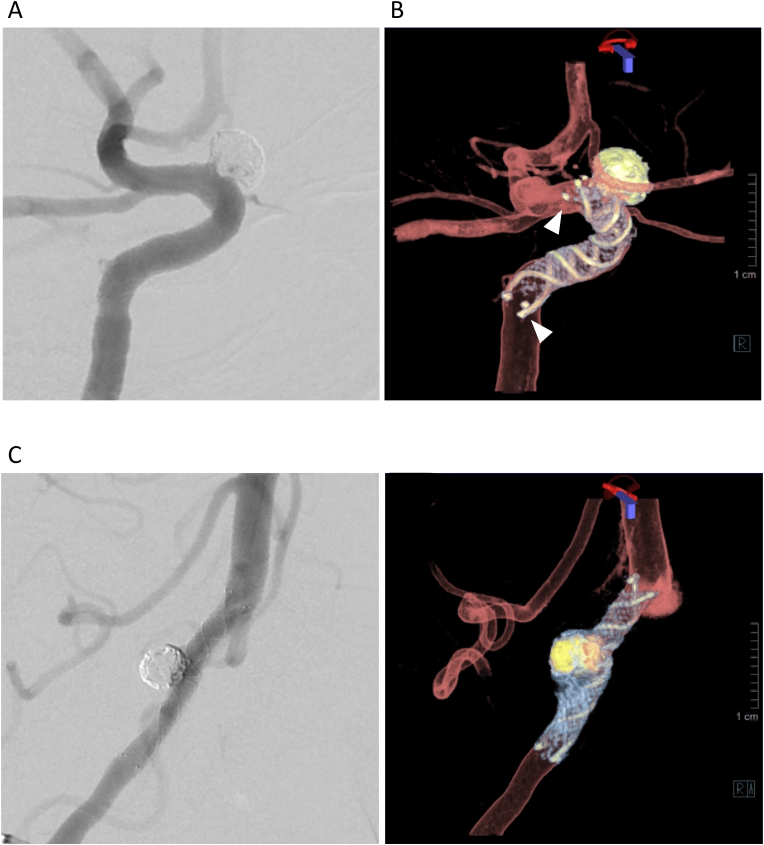
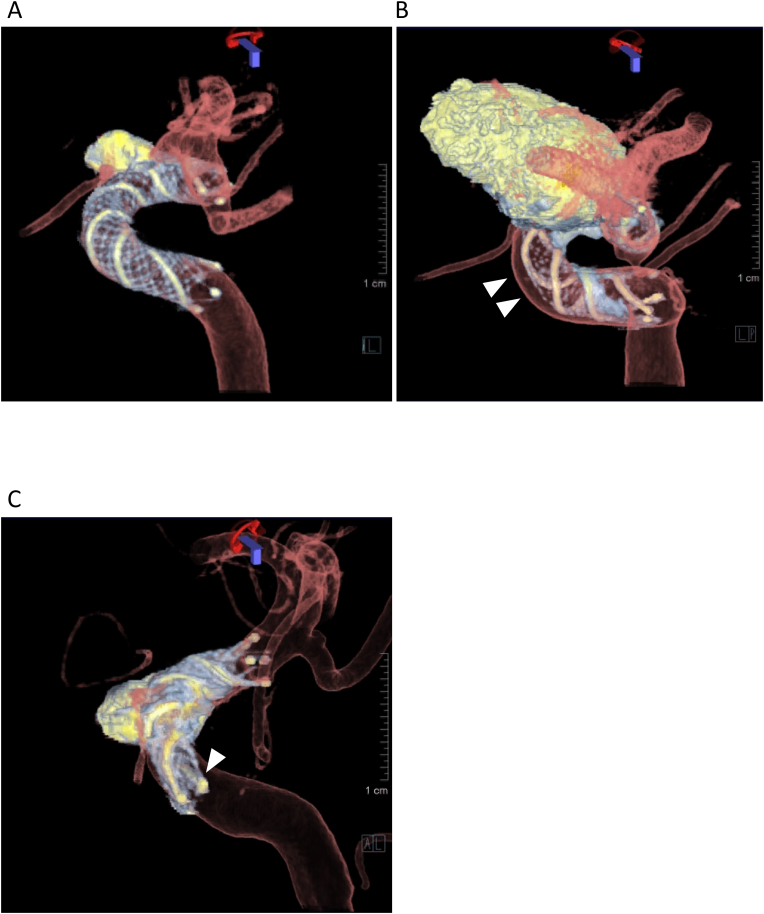
Records of all patients with unruptured intracranial aneurysms who were treated with the LVIS stent were retrospectively accessed and included in this study. Two neurosurgeons evaluated the presence of malapposition between the vessel walls and the stent trunk (crescent sign) and the vessel wall and the stent edges (edge malappostion) on 3D fusion images. These images were high-resolution cone-beam computed tomography images of the LVIS stent fused with 3D-digital subtraction angiography images of the vessels. Associations between malapposition and aneurysm location were assessed by Fisher's exact test, and inter-rater agreement was estimated using Cohen's kappa statistic.
Forty consecutive patients were included. In all patients, 3D fusion imaging successfully visualized the tantalum helical strands and the closed-cell structure of the nitinol material of the low-profile visualized intraluminal support. A crescent sign was observed in 27.5 % and edge malapposition in 47.5 % of the patients. Malapposition was not significantly associated with location ( = 0.23 crescent sign, = 0.07 edge malapposition). Almost perfect ( = 0.88) and substantial ( = 0.76) agreements between the two raters were found for the detection of crescent signs and edge appositions, respectively.
3D fusion imaging provided clear visualization of the LVIS stent and parent arteries, and could detect malapposition with excellent inter-rater reliability. This technique may provide valuable guidance for surgeons in determining postoperative management.
通过三维(3D)融合图像研究低轮廓可视化腔内支撑(LVIS)支架在颅内动脉瘤治疗后的贴合情况,并评估评分者间的可靠性。
回顾性查阅所有接受LVIS支架治疗的未破裂颅内动脉瘤患者的记录,并纳入本研究。两名神经外科医生在3D融合图像上评估血管壁与支架主干之间(新月征)以及血管壁与支架边缘之间(边缘贴合不良)是否存在贴合不良。这些图像是LVIS支架的高分辨率锥形束计算机断层扫描图像与血管的3D数字减影血管造影图像融合而成。通过Fisher精确检验评估贴合不良与动脉瘤位置之间的关联,并使用Cohen卡方统计量估计评分者间的一致性。
连续纳入40例患者。在所有患者中,3D融合成像成功显示了低轮廓可视化腔内支撑的钽螺旋丝和镍钛诺材料的闭孔结构。27.5%的患者观察到新月征,47.5%的患者观察到边缘贴合不良。贴合不良与位置无显著相关性(新月征P = 0.23,边缘贴合不良P = 0.07)。两名评分者在检测新月征和边缘贴合方面的一致性分别为几乎完美(κ = 0.88)和高度一致(κ = 0.76)。
3D融合成像能够清晰显示LVIS支架和供血动脉,并能以优异的评分者间可靠性检测到贴合不良。该技术可为外科医生确定术后管理提供有价值的指导。