Milasinovic Dejan, Tesic Milorad, Nedeljkovic Arsenovic Olga, Maksimovic Ruzica, Sobic Saranovic Dragana, Jelic Dario, Zivkovic Milorad, Dedovic Vladimir, Juricic Stefan, Mehmedbegovic Zlatko, Petrovic Olga, Trifunovic Zamaklar Danijela, Djordjevic Dikic Ana, Giga Vojislav, Boskovic Nikola, Klaric Marija, Zaharijev Stefan, Travica Lazar, Dukic Djordje, Mladenovic Djordje, Asanin Milika, Stankovic Goran
Department of Cardiology, University Clinical Center of Serbia, 11000 Belgrade, Serbia.
Faculty of Medicine, University of Belgrade, 11000 Belgrade, Serbia.
J Clin Med. 2024 Apr 24;13(9):2484. doi: 10.3390/jcm13092484.
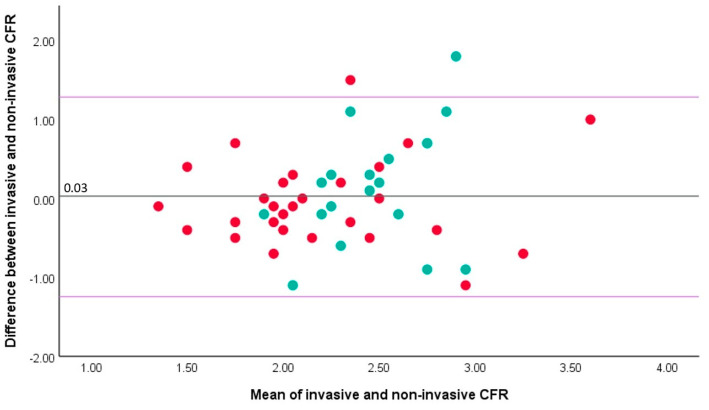
: Coronary microvascular dysfunction is associated with adverse prognosis after ST-segment elevation myocardial infarction (STEMI). We aimed to compare the invasive, Doppler wire-based coronary flow reserve (CFR) with the non-invasive transthoracic Doppler echocardiography (TTDE)-derived CFR, and their ability to predict infarct size. : We included 36 patients with invasive Doppler wire assessment on days 3-7 after STEMI treated with primary percutaneous coronary intervention (PCI), of which TTDE-derived CFR was measured in 47 vessels (29 patients) within 6 h of the invasive Doppler. Infarct size was assessed by cardiac magnetic resonance at a median of 8 months. : The correlation between invasive and non-invasive CFR was modest in the overall cohort (rho 0.400, = 0.005). It improved when only measurements in the LAD artery were considered (rho 0.554, = 0.002), with no significant correlation in the RCA artery (rho -0.190, = 0.435). Both invasive (AUC 0.888) and non-invasive (AUC 0.868) CFR, measured in the recanalized culprit artery, showed a good ability to predict infarct sizes ≥18% of the left ventricular mass, with the optimal cut off values of 1.85 and 1.80, respectively. : In patients with STEMI, TTDE- and Doppler wire-derived CFR exhibit significant correlation, when measured in the LAD artery, and both have a similarly strong association with the final infarct size.
冠状动脉微血管功能障碍与ST段抬高型心肌梗死(STEMI)后的不良预后相关。我们旨在比较基于多普勒导丝的有创冠状动脉血流储备(CFR)和经胸多普勒超声心动图(TTDE)得出的无创CFR,以及它们预测梗死面积的能力。
我们纳入了36例在接受直接经皮冠状动脉介入治疗(PCI)后第3至7天行有创多普勒导丝评估的STEMI患者,其中在有创多普勒检查后6小时内对47支血管(29例患者)测量了经TTDE得出的CFR。在中位数为8个月时通过心脏磁共振评估梗死面积。
在整个队列中,有创和无创CFR之间的相关性一般(rho = 0.400,P = 0.005)。仅考虑左前降支动脉的测量时相关性有所改善(rho = 0.554,P = 0.002),而在右冠状动脉中无显著相关性(rho = -0.190,P = 0.435)。在再通的罪犯血管中测量的有创CFR(AUC = 0.888)和无创CFR(AUC = 0.868)均显示出良好的预测梗死面积≥左心室质量18%的能力,最佳截断值分别为1.85和1.80。
在STEMI患者中,当在左前降支动脉测量时,经TTDE得出的CFR和经多普勒导丝得出的CFR表现出显著相关性,并且两者与最终梗死面积的关联强度相似。