The Cancer Center of the Fifth Affiliated Hospital of Sun Yat-Sen University, Zhuhai, Guangdong Province, 519000, China.
Hangzhou Institute of Medicine (HIM), Zhejiang Cancer Hospital, Chinese Academy of Sciences, Hangzhou, Zhejiang Province, 310022, China.
Cancer Immunol Immunother. 2024 May 11;73(7):125. doi: 10.1007/s00262-024-03698-2.
Despite the success of PD-1 blockade in recurrent/metastatic nasopharyngeal carcinoma (NPC), its effect for locoregionally advanced NPC (LANPC) remains unclear. This study aimed to evaluate the benefit of adding PD-1 blockade to the current standard treatment (gemcitabine and cisplatin IC
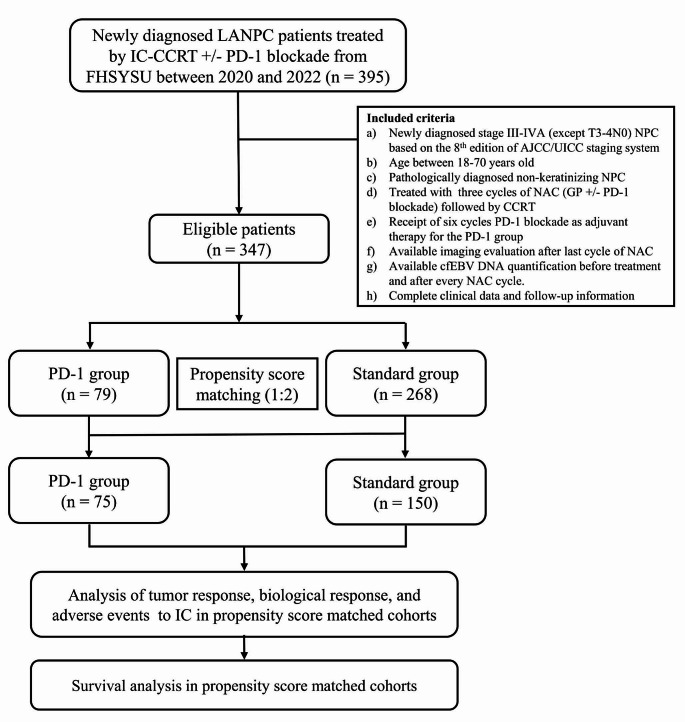
From January 2020 to November 2022, 347 patients with non-metastatic high-risk LANPC (stage III-IVA, excluding T3-4N0) were included. Of the 347 patients, 268 patients were treated with standard treatment (IC-CCRT), and 79 received PD-1 blockade plus IC-CCRT (PD-1 group). For the PD-1 group, PD-1 blockade was given intravenously once every 3 weeks for up to 9 cycles (3 induction and 6 adjuvant). The primary endpoint was disease-free survival (DFS) (i.e. freedom from local/regional/distant failure or death). The propensity score matching (PSM) with the ratio of 1:2 was performed to control confounding factors.
After PSM analysis, 150 patients receiving standard treatment and 75 patients receiving additional PD-1 blockade remained in the current analysis. After three cycles of IC, the PD-1 group had significantly higher rates of complete response (defined as disappearance of all target lesions; 24% vs. 9%; P = 0.006) and complete biological response (defined as undetectable cell-free Epstein-Barr virus DNA, cfEBV DNA; 79% vs. 65%; P = 0.046) than that in the standard group. And the incidence of grade 3-4 toxicity during IC was 47% in the PD-1 group and 41% in the standard group, with no significant difference (P = 0.396). During follow-up period, additional PD-1 blockade to standard treatment improved 3-year DFS from 84 to 95%, with marginal statistical significance (HR, 0.28; 95%CI, 0.06-1.19; P = 0.064).
Additiaonl PD-1 blockade to gemcitabine and cisplatin IC and adjuvant treatment results in significant improvement in tumor regression, cfEBV DNA clearance, superior DFS, and comparable toxicity profiles in high-risk LANPC patients.
尽管 PD-1 阻断在复发性/转移性鼻咽癌(NPC)中取得了成功,但对于局部晚期 NPC(LANPC)的疗效仍不清楚。本研究旨在评估 PD-1 阻断联合当前标准治疗(吉西他滨和顺铂 IC<诱导化疗>加顺铂 CCRT<同期放化疗>)对 LANPC 患者的获益。
本研究纳入了 2020 年 1 月至 2022 年 11 月间 347 例非转移性高危 LANPC(III-IVA 期,不包括 T3-4N0)患者。其中 268 例患者接受标准治疗(IC-CCRT),79 例患者接受 PD-1 阻断联合 IC-CCRT(PD-1 组)。PD-1 组每 3 周静脉注射 PD-1 抑制剂 1 次,最多 9 个周期(3 个诱导周期和 6 个辅助周期)。主要终点是无病生存期(DFS)(即无局部/区域/远处失败或死亡)。采用 1:2 的倾向评分匹配(PSM)以控制混杂因素。
经过 PSM 分析,150 例接受标准治疗的患者和 75 例接受 PD-1 阻断联合治疗的患者仍纳入本研究。在 IC 治疗 3 个周期后,PD-1 组完全缓解(定义为所有靶病灶消失;24% vs. 9%;P=0.006)和完全生物反应(定义为无法检测到游离 Epstein-Barr 病毒 DNA,cfEBV DNA;79% vs. 65%;P=0.046)的比例显著高于标准组。IC 期间 3-4 级毒性的发生率在 PD-1 组为 47%,在标准组为 41%,差异无统计学意义(P=0.396)。在随访期间,与标准治疗相比,LANPC 高危患者加用 PD-1 阻断可使 3 年 DFS 从 84%提高至 95%,具有边缘统计学意义(HR,0.28;95%CI,0.06-1.19;P=0.064)。
在高危 LANPC 患者中,吉西他滨和顺铂 IC 联合辅助治疗加用 PD-1 阻断可显著提高肿瘤消退率、cfEBV DNA 清除率、DFS,并具有可比较的毒性特征。