Caboolture Hospital, Caboolture, Australia.
James Mayne Academy of Critical Care, The University of Queensland, Brisbane, Australia.
PLoS One. 2024 May 13;19(5):e0295347. doi: 10.1371/journal.pone.0295347. eCollection 2024.
When clinicians need to administer a vasopressor infusion, they are faced with the choice of administration via either peripheral intravenous catheter (PIVC) or central venous catheter (CVC). Vasopressor infusions have traditionally been administered via central venous catheters (CVC) rather than Peripheral Intra Venous Catheters (PIVC), primarily due to concerns of extravasation and resultant tissue injury. This practice is not guided by contemporary randomised controlled trial (RCT) evidence. Observational data suggests safety of vasopressor infusion via PIVC. To address this evidence gap, we have designed the "Vasopressors Infused via Peripheral or Central Access" (VIPCA) RCT.
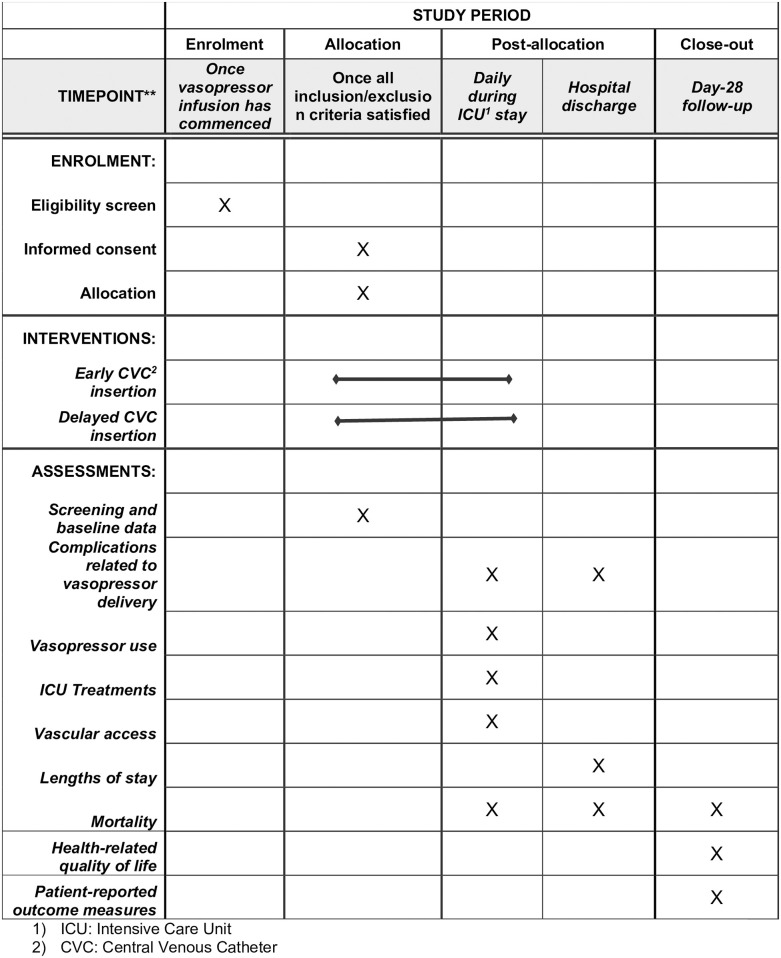
The VIPCA trial is a single-centre, feasibility, parallel-group RCT. Eligible critically ill patients requiring a vasopressor infusion will be identified by emergency department (ED) or intensive care unit (ICU) staff and randomised to receive vasopressor infusion via either PIVC or CVC. Primary outcome is feasibility, a composite of recruitment rate, proportion of eligible patients randomised, protocol fidelity, retention and missing data. Primary clinical outcome is days alive and out of hospital up to day-30. Secondary outcomes will include safety and other clinical outcomes, and process and cost measures. Specific aspects of safety related to vasopressor infusions such as extravasation, leakage, device failure, tissue injury and infection will be assessed.
VIPCA is a feasibility RCT whose outcomes will inform the feasibility and design of a multicentre Phase-3 trial comparing routes of vasopressor delivery. The exploratory economic analysis will provide input data for the full health economic analysis which will accompany any future Phase-3 RCT.
当临床医生需要进行血管加压素输注时,他们面临着通过外周静脉导管(PIVC)或中心静脉导管(CVC)进行给药的选择。血管加压素输注传统上通过中心静脉导管(CVC)而不是外周静脉内导管(PIVC)进行,主要是因为担心外渗和由此导致的组织损伤。这种做法没有得到当代随机对照试验(RCT)证据的指导。观察性数据表明,通过 PIVC 输注血管加压素是安全的。为了解决这一证据差距,我们设计了“通过外周或中央通路输注血管加压素”(VIPCA)RCT。
VIPCA 试验是一项单中心、可行性、平行组 RCT。急诊科(ED)或重症监护病房(ICU)工作人员将确定需要血管加压素输注的危重症患者,并将其随机分为通过 PIVC 或 CVC 接受血管加压素输注。主要结局是可行性,包括招募率、随机分组的合格患者比例、方案一致性、保留率和缺失数据的综合指标。主要临床结局是存活且出院的天数,截止到第 30 天。次要结局将包括安全性和其他临床结局,以及过程和成本措施。将评估与血管加压素输注相关的特定安全性方面,如外渗、渗漏、设备故障、组织损伤和感染。
VIPCA 是一项可行性 RCT,其结果将为比较血管加压素输送途径的多中心 3 期试验的可行性和设计提供信息。探索性经济分析将为伴随任何未来 3 期 RCT 的全面健康经济分析提供输入数据。