Dartmouth Health, Department of Orthopaedics, Lebanon, New Hampshire, United States.
Dartmouth College, Geisel School of Medicine, Hanover, New Hampshire, United States.
J Biomed Opt. 2024 Jun;29(6):066003. doi: 10.1117/1.JBO.29.6.066003. Epub 2024 May 14.
Necrotizing soft-tissue infections (NSTIs) are life-threatening infections with a cumulative case fatality rate of 21%. The initial presentation of an NSTI is non-specific, frequently leading to misdiagnosis and delays in care. No current strategies yield an accurate, real-time diagnosis of an NSTI.
A first-in-kind, observational, clinical pilot study tested the hypothesis that measurable fluorescence signal voids occur in NSTI-affected tissues following intravenous administration and imaging of perfusion-based indocyanine green (ICG) fluorescence. This hypothesis is based on the established knowledge that NSTI is associated with local microvascular thrombosis.
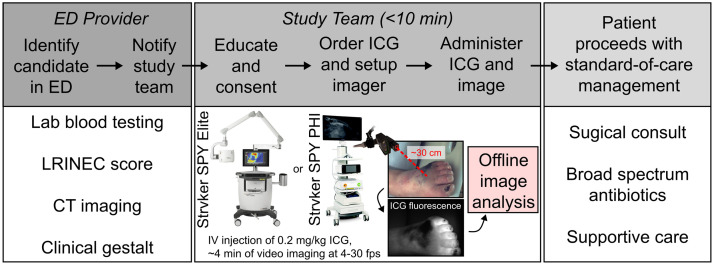
Adult patients presenting to the Emergency Department of a tertiary care medical center at high risk for NSTI were prospectively enrolled and imaged with a commercial fluorescence imager. Single-frame fluorescence snapshot and first-pass perfusion kinetic parameters-ingress slope (IS), time-to-peak (TTP) intensity, and maximum fluorescence intensity (IMAX)-were quantified using a dynamic contrast-enhanced fluorescence imaging technique. Clinical variables (comorbidities, blood laboratory values), fluorescence parameters, and fluorescence signal-to-background ratios (SBRs) were compared to final infection diagnosis.
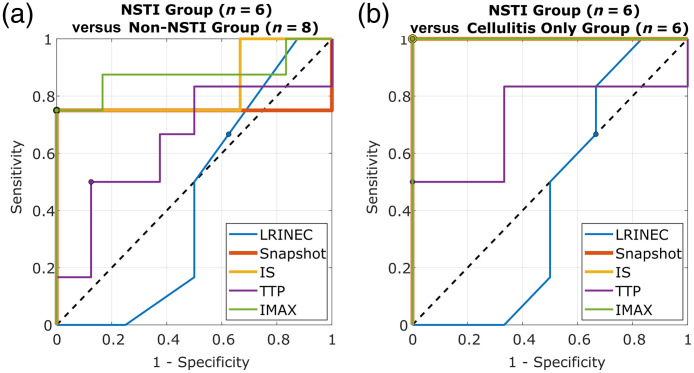
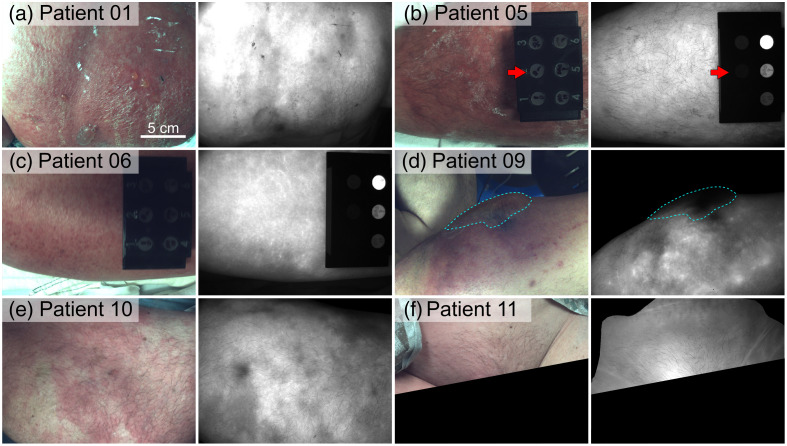
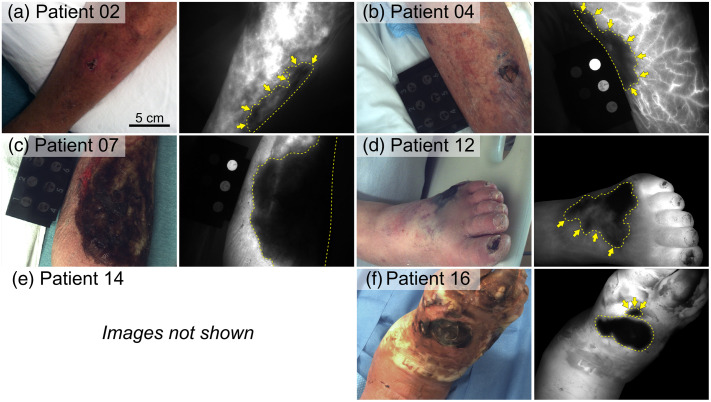
Fourteen patients were enrolled and imaged (six NSTI, six cellulitis, one diabetes mellitus-associated gangrene, and one osteomyelitis). Clinical variables demonstrated no statistically significant differences between NSTI and non-NSTI patient groups (). All NSTI cases exhibited prominent fluorescence signal voids in affected tissues, including tissue features not visible to the naked eye. All cellulitis cases exhibited a hyperemic response with increased fluorescence and no distinct signal voids. Median lesion-to-background tissue SBRs based on snapshot, IS, TTP, and IMAX parameter maps ranged from 3.2 to 9.1, 2.2 to 33.8, 1.0 to 7.5, and 1.5 to 12.7, respectively, for the NSTI patient group. All fluorescence parameters except TTP demonstrated statistically significant differences between NSTI and cellulitis patient groups ().
Real-time, accurate discrimination of NSTIs compared with non-necrotizing infections may be possible with perfusion-based ICG fluorescence imaging.
坏死性软组织感染(NSTI)是一种危及生命的感染,累积病死率为 21%。NSTI 的初始表现是非特异性的,常导致误诊和治疗延误。目前尚无策略能准确、实时地诊断 NSTI。
首例观察性临床试点研究检验了这样一个假设,即在静脉注射和灌注型吲哚菁绿(ICG)荧光成像后,NSTI 受累组织会出现可测量的荧光信号缺失。这一假设基于这样一个既定的知识,即 NSTI 与局部微血管血栓形成有关。
将高风险 NSTI 的成年患者前瞻性纳入三级医疗中心的急诊科,并使用商业荧光成像仪进行成像。使用动态对比增强荧光成像技术,对单帧荧光快照和首过灌注动力学参数(入口斜率[IS]、达峰时间[TTP]强度和最大荧光强度[IMAX])进行量化。临床变量(合并症、血液实验室值)、荧光参数和荧光信号与背景比值(SBR)与最终感染诊断进行比较。
共纳入并成像了 14 例患者(6 例 NSTI、6 例蜂窝织炎、1 例糖尿病相关坏疽和 1 例骨髓炎)。临床变量在 NSTI 和非 NSTI 患者组之间无统计学显著差异()。所有 NSTI 病例均在受累组织中表现出明显的荧光信号缺失,包括肉眼不可见的组织特征。所有蜂窝织炎病例均表现出荧光增强的充血反应,无明显的信号缺失。基于快照、IS、TTP 和 IMAX 参数图的病变与背景组织 SBR 的中位数范围分别为 3.2 至 9.1、2.2 至 33.8、1.0 至 7.5 和 1.5 至 12.7,用于 NSTI 患者组。NSTI 和蜂窝织炎患者组之间,除 TTP 外,所有荧光参数均有统计学显著差异()。
基于 ICG 荧光灌注成像,可能可以实时、准确地区分 NSTI 与非坏死性感染。