Adhil Ibrahim, Dahal Suman, Gyawali Sushil, Neupane Prashansha, Kharel Ashok, Neupane Priyanka, Pachhai Prarthana, Khadka Rabi, Khatiwada Raj D, Shrestha Jayan M
Department of General Surgery.
Karnali Academy of Health Sciences, Jumla, Nepal.
Ann Med Surg (Lond). 2023 Nov 1;85(12):5874-5878. doi: 10.1097/MS9.0000000000001447. eCollection 2023 Dec.
From its historical identification to modern times with advancements in management modalities globally, the mortality of necrotizing fasciitis (NF) is high ranging from 19 to 30% for all affected sites. Although many diagnostic adjuncts have been developed to assist with the prompt and accurate diagnosis of NF, the primary diagnosis is still based on high clinical suspicion. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was developed as a tool for distinguishing NF from other soft tissue infections. The main objective of this study is to evaluate LRINEC as a tool for early diagnosis of NF and differentiating it from other soft tissue infections like cellulitis.
This is a single-centered, prospective observational study. Patients presenting with soft tissue infections of the limbs to the emergency department from November 2020 to October 2021 were included in this study. The clinical findings and blood parameters for the LRINEC score were collected and the score was calculated. Based on clinical suspicion of NF, patients underwent debridement and had a tissue biopsy to confirm the diagnosis. The data obtained was analyzed using SPSS version 24 and MS Excel. The AUC curve was used to calculate a cutoff, sensitivity, specificity, positive predictive value, and negative predictive values for the LRINEC score based on our study.
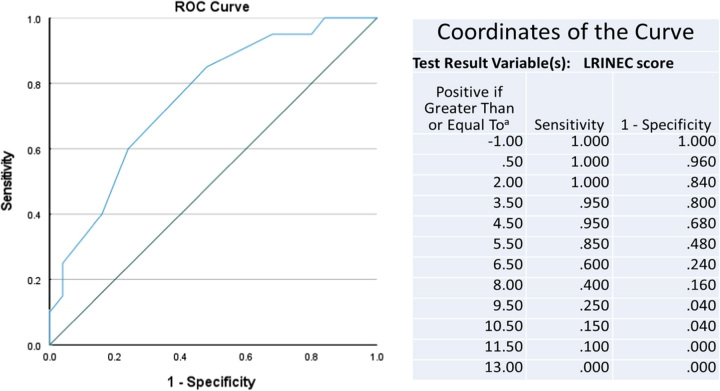
Forty-five patients with 28 males and 17 females were included. The average age was 53.667 years within a range of 19-79 years. Among them 44.4% of the patients had NF and 66.6% had other minor forms of soft tissue infections. The ROC curve obtained a cutoff value of greater than or equal to 6, with an AUC of 0.751. At this cut of value study showed a sensitivity of 85% with a specificity of 52%. Similarly, positive predictive value was found to be 58.62%, negative predictive values of 81.25%, and overall accuracy of 66.67% in early diagnosis of NF.
In conclusion, our study showed that the LRINEC score can be a reliable tool for the early diagnosis of NF in an ED setting. This scoring system is best to be used to rule out NF.
从坏死性筋膜炎(NF)的历史确认到现代,随着全球管理方式的进步,NF的死亡率仍然很高,所有受累部位的死亡率在19%至30%之间。尽管已经开发了许多辅助诊断方法来帮助快速准确地诊断NF,但主要诊断仍基于高度的临床怀疑。坏死性筋膜炎实验室风险指标(LRINEC)评分作为一种区分NF与其他软组织感染的工具而被开发出来。本研究的主要目的是评估LRINEC作为NF早期诊断以及将其与蜂窝织炎等其他软组织感染区分开来的工具。
这是一项单中心前瞻性观察研究。纳入了2020年11月至2021年10月期间到急诊科就诊的肢体软组织感染患者。收集LRINEC评分的临床发现和血液参数并计算该评分。基于对NF的临床怀疑,患者接受清创术并进行组织活检以确诊。使用SPSS 24版和MS Excel对获得的数据进行分析。根据我们的研究,利用AUC曲线计算LRINEC评分的临界值、敏感性、特异性、阳性预测值和阴性预测值。
共纳入45例患者,其中男性28例女性17例。平均年龄为53.667岁,年龄范围在19至79岁之间。其中44.4%的患者患有NF,66.6%的患者患有其他轻度软组织感染形式。ROC曲线获得的临界值大于或等于6,AUC为0.751。在这个临界值下,研究显示敏感性为85%,特异性为52%。同样,在NF的早期诊断中,阳性预测值为58.62%,阴性预测值为81.25%,总体准确率为66.67%。
总之,我们的研究表明,LRINEC评分可作为急诊科环境中NF早期诊断的可靠工具。该评分系统最适合用于排除NF。