Peketi Sindhu Harika, Upadrista Pratap Kumar, Cadet Bair, Cadet Johanne, Cadet Noonkee
Internal Medicine, Nassau University Medical Center, East Meadow, USA.
Nephrology, Nassau University Medical Center, East Meadow, USA.
Cureus. 2024 May 13;16(5):e60241. doi: 10.7759/cureus.60241. eCollection 2024 May.
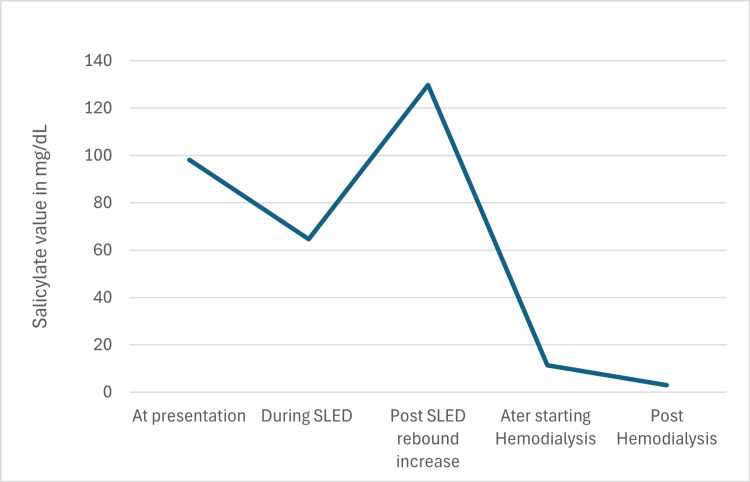
Salicylate exposure and toxicity are associated with a myriad of symptoms and signs, and a comprehensive knowledge of diagnosing and treating salicylate poisoning is needed. Here, we present a case of a 29-year-old female with a past medical history of schizoaffective disorder and bipolar disorder with multiple suicide attempts brought to our hospital, Nassau University Medical Center, East Meadow, by the Emergency Medical Service (EMS) due to an intentional overdose of 300 pills of acetylsalicylic acid. She had mixed acid-base disturbance with respiratory alkalosis and metabolic acidosis. She was started on bicarbonate infusion in the emergency department to maintain a blood pH of 7.5 and to maintain a urine pH of more than 7.5. As her salicylate levels were 98.2 at admission with altered mental status, she was started on slow, low-efficiency hemodialysis. A few hours later, she developed a rebound increase in salicylate levels to 129, associated with a change in mental status and the patient was more confused. She was started on regular hemodialysis with improvement in mental status and elimination of salicylate steadily. Given the extensive nature of toxic effects, a patient with severe salicylate toxicity can deteriorate rapidly and can be challenging to manage. As there is no specific antidote for aspirin, the goals of therapy depend primarily on limiting the absorption of salicylate, enhancing elimination, and providing supportive care. Monitoring the acid-base status and serum salicylate levels closely and monitoring for rebound increase in salicylate levels is of paramount importance. Aggressive hydration to maintain euvolemia, alkalinization, aggressive replenishment of potassium and magnesium, activated charcoal to decrease absorption, and hemodialysis remain the cornerstones of treatment.
水杨酸盐暴露与中毒会引发众多症状和体征,因此需要全面了解水杨酸盐中毒的诊断与治疗方法。在此,我们呈现一例29岁女性病例,该患者有精神分裂情感障碍和双相情感障碍病史,曾多次尝试自杀,因故意过量服用300片乙酰水杨酸被紧急医疗服务(EMS)送至我们位于东梅多的拿骚大学医学中心。她存在混合性酸碱紊乱,伴有呼吸性碱中毒和代谢性酸中毒。在急诊科,她开始接受碳酸氢盐输注,以维持血液pH值为7.5,并使尿液pH值保持在7.5以上。由于入院时她的水杨酸盐水平为98.2且精神状态改变,遂开始进行缓慢、低效的血液透析。数小时后,她的水杨酸盐水平反弹至129,精神状态也发生变化,更加混乱。随后她开始接受常规血液透析,精神状态有所改善,水杨酸盐也稳步清除。鉴于中毒影响范围广泛,重度水杨酸盐中毒患者病情可能迅速恶化,治疗颇具挑战性。由于阿司匹林没有特效解毒剂,治疗目标主要是限制水杨酸盐的吸收、促进清除并提供支持性护理。密切监测酸碱状态和血清水杨酸盐水平,并监测水杨酸盐水平的反弹升高至关重要。积极补液以维持血容量正常、碱化尿液、积极补充钾和镁、使用活性炭减少吸收以及进行血液透析仍是治疗的基石。