Caplan Avrom S, Todd Gabrielle C, Zhu YanChun, Sikora Michelle, Akoh Christine C, Jakus Jeannette, Lipner Shari R, Graber Kayla Babbush, Acker Karen P, Morales Ayana E, Rolón Rebecca M Marrero, Westblade Lars F, Fonseca Maira, Cline Abigail, Gold Jeremy A W, Lockhart Shawn R, Smith Dallas J, Chiller Tom, Greendyke William G, Manjari Swati R, Banavali Nilesh K, Chaturvedi Sudha
The Ronald O. Perelman Department of Dermatology, NYU Grossman School of Medicine, New York, New York.
Dermatology Service, Bellevue Hospital Center, New York, New York.
JAMA Dermatol. 2024 Jul 1;160(7):701-709. doi: 10.1001/jamadermatol.2024.1126.
Trichophyton indotineae is an emerging dermatophyte causing outbreaks of extensive tinea infections often unresponsive to terbinafine. This species has been detected worldwide and in multiple US states, yet detailed US data on infections with T indotineae are sparse and could improve treatment practices and medical understanding of transmission.
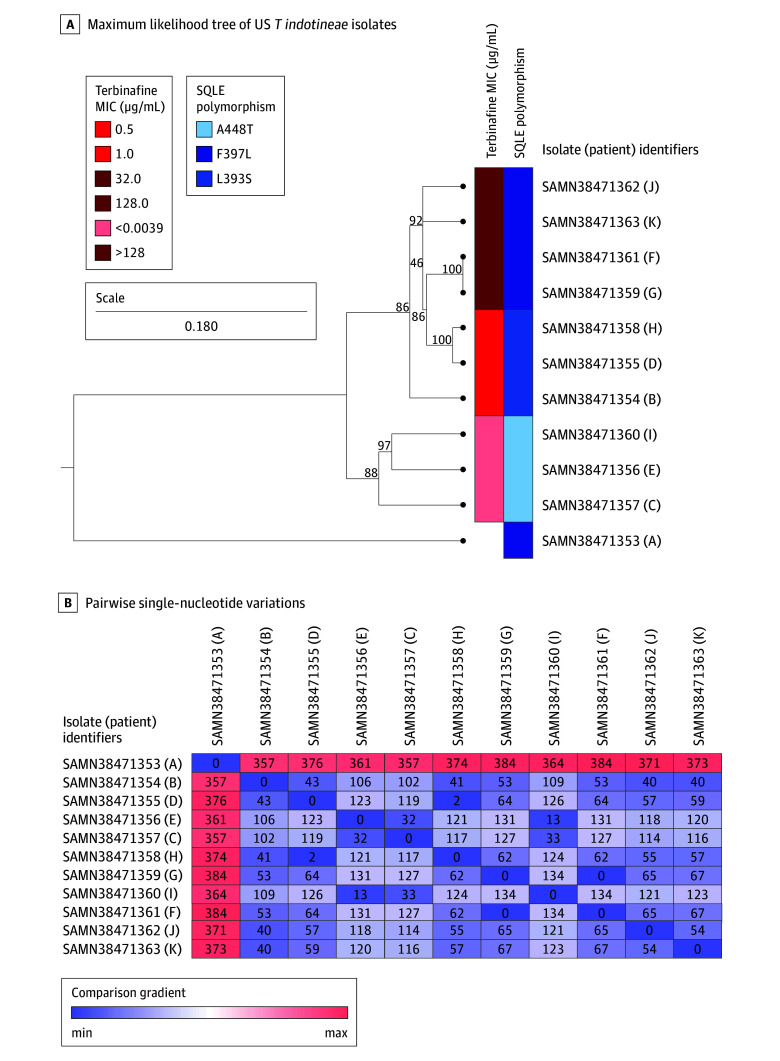
To correlate clinical features of T indotineae infections with in vitro antifungal susceptibility testing results, squalene epoxidase gene sequence variations, and isolate relatedness using whole-genome sequencing.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study of patients with T indotineae infections in New York City spanned May 2022 to May 2023. Patients with confirmed T indotineae infections were recruited from 6 New York City medical centers.
Improvement or resolution at the last follow-up assessment.
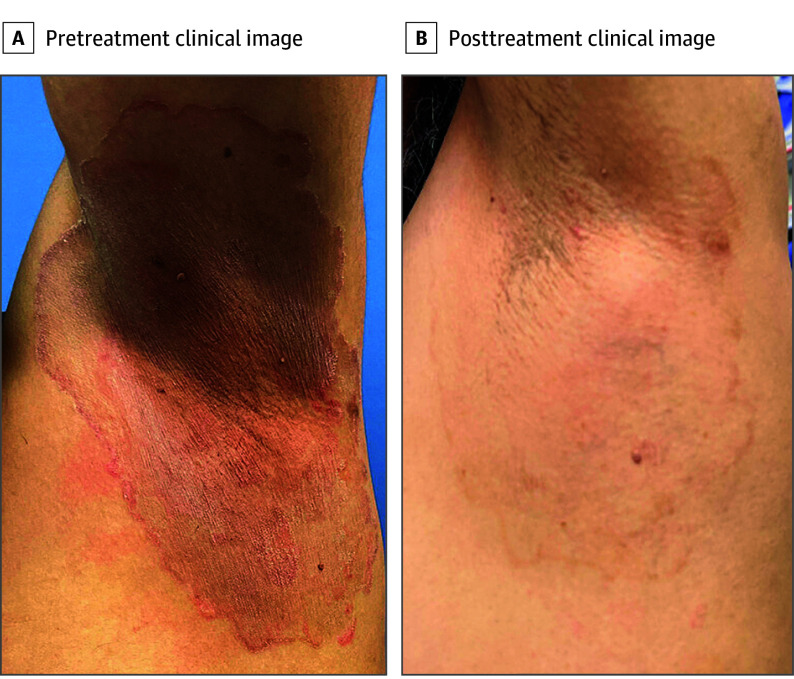
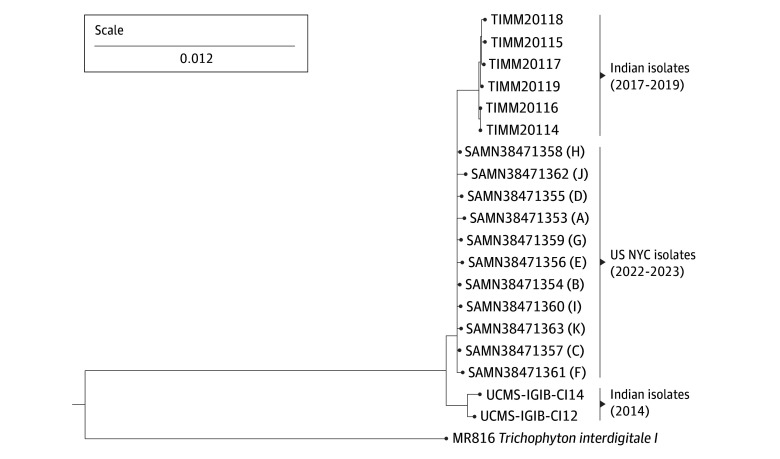
Among 11 patients with T indotineae (6 male and 5 female patients; median [range] age, 39 [10-65] years), 2 were pregnant; 1 had lymphoma; and the remainder were immunocompetent. Nine patients reported previous travel to Bangladesh. All had widespread lesions with variable scale and inflammation, topical antifungal monotherapy failure, and diagnostic delays (range, 3-42 months). Terbinafine treatment failed in 7 patients at standard doses (250 mg daily) for prolonged duration; these patients also had isolates with amino acid substitutions at positions 393 (L393S) or 397 (F397L) in squalene epoxidase that correlated with elevated terbinafine minimum inhibitory concentrations of 0.5 μg/mL or higher. Patients who were treated with fluconazole and griseofulvin improved in 2 of 4 and 2 of 5 instances, respectively, without correlation between outcomes and antifungal minimum inhibitory concentrations. Furthermore, 5 of 7 patients treated with itraconazole cleared or had improvement at the last follow-up, and 2 of 7 were lost to follow-up or stopped treatment. Based on whole-genome sequencing analysis, US isolates formed a cluster distinct from Indian isolates.
The results of this case series suggest that disease severity, diagnostic delays, and lack of response to typically used doses and durations of antifungals for tinea were common in this primarily immunocompetent patient cohort with T indotineae, consistent with published data. Itraconazole was generally effective, and the acquisition of infection was likely in Bangladesh.
印多蒂内毛癣菌是一种新出现的皮肤癣菌,可引起广泛的癣感染暴发,通常对特比萘芬无反应。该菌种已在全球和美国多个州被检测到,但美国关于印多蒂内毛癣菌感染的详细数据稀少,而这些数据可改善治疗方法并增进对传播的医学理解。
将印多蒂内毛癣菌感染的临床特征与体外抗真菌药敏试验结果、角鲨烯环氧酶基因序列变异以及使用全基因组测序的菌株相关性进行关联。
设计、地点和参与者:这项对纽约市印多蒂内毛癣菌感染患者的回顾性队列研究涵盖2022年5月至2023年5月。确诊为印多蒂内毛癣菌感染的患者从纽约市的6个医疗中心招募。
最后一次随访评估时的改善或缓解情况。
在11例印多蒂内毛癣菌感染患者中(6例男性和5例女性患者;中位[范围]年龄为39[10 - 65]岁),2例为孕妇;1例患有淋巴瘤;其余患者免疫功能正常。9例患者报告此前去过孟加拉国。所有患者均有广泛的皮损,皮损范围和炎症程度各异,局部抗真菌单药治疗失败,且诊断延迟(范围为3 - 42个月)。7例患者接受标准剂量(每日250 mg)的特比萘芬治疗较长时间后失败;这些患者的角鲨烯环氧酶在393位(L393S)或397位(F397L)有氨基酸替换的菌株,这与特比萘芬最低抑菌浓度升高至0.5μg/mL或更高相关。接受氟康唑和灰黄霉素治疗的患者分别在4例中的2例和5例中的2例有所改善,结局与抗真菌最低抑菌浓度之间无相关性。此外,接受伊曲康唑治疗的7例患者中有5例在最后一次随访时清除感染或病情改善,7例中有2例失访或停止治疗。基于全基因组测序分析,美国的分离菌株形成了一个与印度分离菌株不同的聚类。
该病例系列的结果表明,在这个以免疫功能正常为主的印多蒂内毛癣菌感染患者队列中,疾病严重程度、诊断延迟以及对癣常用剂量和疗程的抗真菌药物无反应的情况很常见,这与已发表的数据一致。伊曲康唑总体有效,感染可能是在孟加拉国获得的。