Department of Medicine, University of Ottawa, Ottawa, ON, Canada.
Department of Medicine, University of Toronto, Toronto, Ontario, ON, Canada.
BMC Gastroenterol. 2024 May 17;24(1):172. doi: 10.1186/s12876-024-03226-7.
Hospital re-admission for persons with Crohn's disease (CD) is a significant contributor to morbidity and healthcare costs. We derived prediction models of risk of 90-day re-hospitalization among persons with CD that could be applied at hospital discharge to target outpatient interventions mitigating this risk.
We performed a retrospective study in persons with CD admitted between 2009 and 2016 for an acute CD-related indication. Demographic, clinical, and health services predictor variables were ascertained through chart review and linkage to administrative health databases. We derived and internally validated a multivariable logistic regression model of 90-day CD-related re-hospitalization. We selected the optimal probability cut-point to maximize Youden's index.
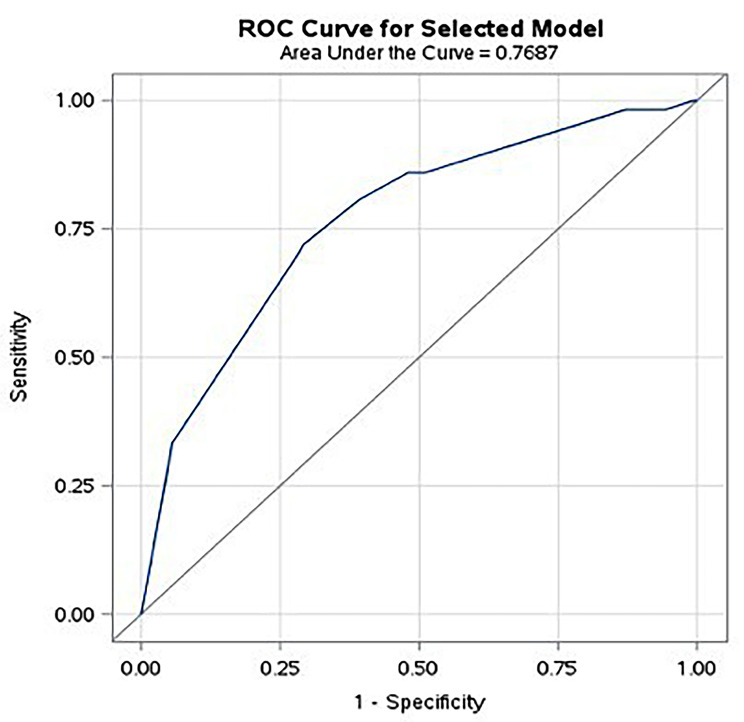
There were 524 CD hospitalizations and 57 (10.9%) CD re-hospitalizations within 90 days of discharge. Our final model included hospitalization within the prior year (adjusted odds ratio [aOR] 3.27, 95% confidence interval [CI] 1.76-6.08), gastroenterologist consultation within the prior year (aOR 0.185, 95% CI 0.0950-0.360), intra-abdominal surgery during index hospitalization (aOR 0.216, 95% CI 0.0500-0.934), and new diagnosis of CD during index hospitalization (aOR 0.327, 95% CI 0.0950-1.13). The model demonstrated good discrimination (optimism-corrected c-statistic value 0.726) and excellent calibration (Hosmer-Lemeshow goodness-of-fit p-value 0.990). The optimal model probability cut point allowed for a sensitivity of 71.9% and specificity of 70.9% for identifying 90-day re-hospitalization, at a false positivity rate of 29.1% and false negativity rate of 28.1%.
Demographic, clinical, and health services variables can help discriminate persons with CD at risk of early re-hospitalization, which could permit targeted post-discharge intervention.
克罗恩病(CD)患者的住院再入院是发病率和医疗保健成本的重要因素。我们得出了 CD 患者 90 天再入院风险的预测模型,这些模型可以在出院时应用,以针对减轻这种风险的门诊干预措施。
我们对 2009 年至 2016 年间因急性 CD 相关原因住院的 CD 患者进行了回顾性研究。通过病历回顾和与行政健康数据库的链接,确定了人口统计学、临床和卫生服务预测变量。我们推导出并内部验证了一个 90 天 CD 相关再入院的多变量逻辑回归模型。我们选择了最优的概率截断点,以最大化 Youden 指数。
共有 524 例 CD 住院和 57 例(10.9%)CD 患者在出院后 90 天内再住院。我们的最终模型包括前一年的住院治疗(调整后的优势比[aOR]3.27,95%置信区间[CI]1.76-6.08),前一年的胃肠病医生咨询(aOR 0.185,95%CI 0.0950-0.360),指数住院期间的腹腔内手术(aOR 0.216,95%CI 0.0500-0.934)和指数住院期间新诊断的 CD(aOR 0.327,95%CI 0.0950-1.13)。该模型显示出良好的区分度(校正后的乐观 c 统计值为 0.726)和出色的校准度(Hosmer-Lemeshow 拟合优度检验 p 值为 0.990)。最优模型概率截断点可以识别 90 天再入院,其敏感性为 71.9%,特异性为 70.9%,假阳性率为 29.1%,假阴性率为 28.1%。
人口统计学、临床和卫生服务变量可以帮助识别有早期再入院风险的 CD 患者,从而可以进行有针对性的出院后干预。