Rheumatology and Clinical Immunology Unit, Attikon University Hospital, National and Kapodistrian University of Athens School of Medicine, Athens, Greece.
Vasculitis Service, Rheumatology Department, Norfolk and Norwich University Hospital NHS Trust, Norwich, UK.
Ann Rheum Dis. 2024 Oct 21;83(11):1489-1501. doi: 10.1136/ard-2023-225319.
To analyse the new evidence (2018-2022) for the management of systemic lupus erythematosus (SLE) to inform the 2023 update of the European League Against Rheumatism (EULAR) recommendations.
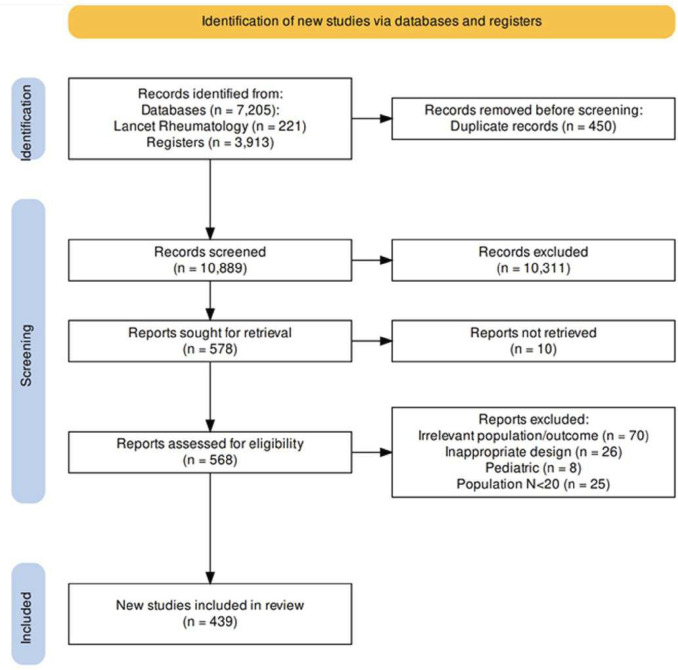
Systematic literature reviews were performed in the Medline and the Cochrane Library databases capturing publications from 1 January 2018 through 31 December 2022, according to the EULAR standardised operating procedures. The research questions focused on five different domains, namely the benefit/harm of SLE treatments, the benefits from the attainment of remission/low disease activity, the risk/benefit from treatment tapering/withdrawal, the management of SLE with antiphospholipid syndrome and the safety of immunisations against varicella zoster virus and SARS-CoV2 infection. A Population, Intervention, Comparison and Outcome framework was used to develop search strings for each research topic.
We identified 439 relevant articles, the majority being observational studies of low or moderate quality. High-quality randomised controlled trials (RCTs) documented the efficacy of the type 1 interferon receptor inhibitor, anifrolumab, in non-renal SLE, and belimumab and voclosporin, a novel calcineurin inhibitor, in lupus nephritis (LN), when compared with standard of care. For the treatment of specific organ manifestations outside LN, a lack of high-quality data was documented. Multiple observational studies confirmed the beneficial effects of attaining clinical remission or low disease activity, reducing the risk for multiple adverse outcomes. Two randomised trials with some concerns regarding risk of bias found higher rates of relapse in patients who discontinued glucocorticoids (GC) or immunosuppressants in SLE and LN, respectively, yet observational cohort studies suggest that treatment withdrawal might be feasible in a subset of patients.
Anifrolumab and belimumab achieve better disease control than standard of care in extrarenal SLE, while combination therapies with belimumab and voclosporin attained higher response rates in high-quality RCTs in LN. Remission and low disease activity are associated with favourable long-term outcomes. In patients achieving these targets, GC and immunosuppressive therapy may gradually be tapered. Cite Now.
分析 2018-2022 年系统性红斑狼疮(SLE)管理的新证据,为 2023 年更新欧洲抗风湿病联盟(EULAR)建议提供信息。
根据 EULAR 标准化操作程序,在 Medline 和 Cochrane 图书馆数据库中进行了系统性文献综述,以获取 2018 年 1 月 1 日至 2022 年 12 月 31 日的出版物。研究问题集中在五个不同领域,即 SLE 治疗的获益/危害、达到缓解/低疾病活动的获益、治疗减量/停药的风险/获益、抗磷脂综合征合并 SLE 的治疗以及水痘带状疱疹病毒和 SARS-CoV2 感染疫苗的安全性。使用人群、干预、比较和结局框架为每个研究主题开发了搜索字符串。
我们确定了 439 篇相关文章,其中大多数是低质量或中等质量的观察性研究。高质量的随机对照试验(RCT)记录了 1 型干扰素受体抑制剂 anifrolumab 在非肾 SLE 中的疗效,以及新型钙调神经磷酸酶抑制剂 belimumab 和 voclosporin 在狼疮肾炎(LN)中的疗效,与标准治疗相比。对于 LN 以外的特定器官表现的治疗,缺乏高质量的数据。多项观察性研究证实了达到临床缓解或低疾病活动的有益效果,降低了多种不良结局的风险。两项存在偏倚风险的随机试验发现,停止糖皮质激素(GC)或免疫抑制剂治疗的 SLE 和 LN 患者的复发率更高,而观察性队列研究表明,在某些患者中可能可以进行治疗停药。
在非肾 SLE 中,anifrolumab 和 belimumab 比标准治疗能更好地控制疾病,而 belimumab 和 voclosporin 的联合治疗在高质量 RCT 中在 LN 中获得了更高的反应率。缓解和低疾病活动与有利的长期结局相关。在达到这些目标的患者中,GC 和免疫抑制治疗可能逐渐减少。