Lewek Joanna, Bielecka-Dąbrowa Agata, Toth Peter P, Banach Maciej
Department of Preventive Cardiology and Lipidology, Medical University of Lodz (MUL), Rzgowska 281/289, 93-338 Lodz, Poland.
Department of Cardiology and Congenital Diseases of Adults, Polish Mother's Memorial Hospital Research Institute (PMMHRI), Rzgowska 281/289, 93-338 Lodz, Poland.
Eur Heart J Open. 2024 Apr 26;4(3):oeae032. doi: 10.1093/ehjopen/oeae032. eCollection 2024 May.
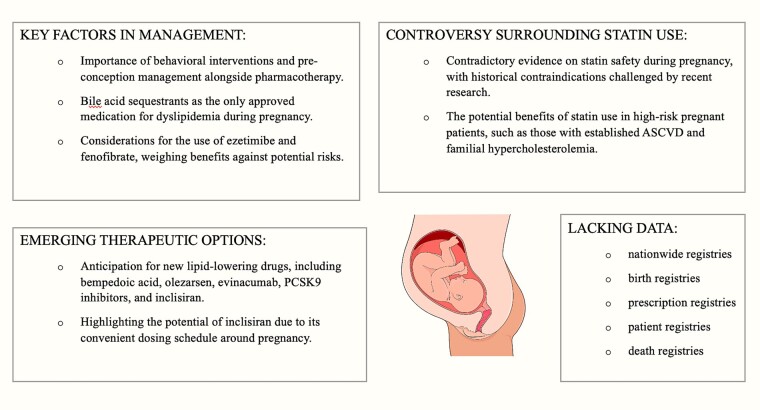
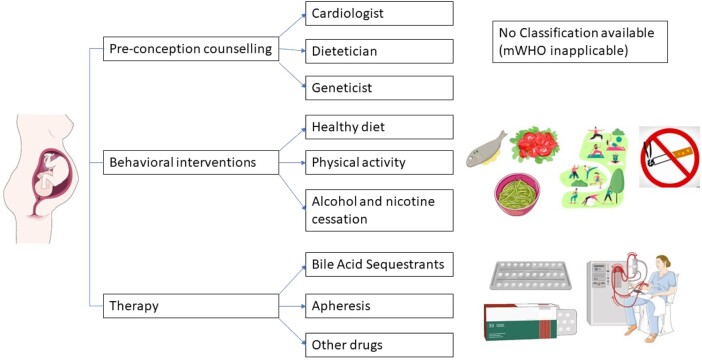
Over several decades, the approach to treating dyslipidaemias during pregnancy remains essentially unchanged. The lack of advancement in this field is mostly related to the fact that we lack clinical trials of pregnant patients both with available as well as new therapies. While there are numerous novel therapies developed for non-pregnant patients, there are still many limitations in dyslipidaemia treatment during pregnancy. Besides pharmacotherapy and careful clinical assessment, the initiation of behavioural modifications as well as pre-conception management is very important. Among the various lipid-lowering medications, bile acid sequestrants are the only ones officially approved for treating dyslipidaemia in pregnancy. Ezetimibe and fenofibrate can be considered if their benefits outweigh potential risks. Statins are still considered contraindicated, primarily due to animal studies and human case reports. However, recent systematic reviews and meta-analyses as well as data on familial hypercholesterolaemia (FH) in pregnant patients have indicated that their use may not be harmful and could even be beneficial in certain selected cases. This is especially relevant for pregnant patients at very high cardiovascular risk, such as those who have already experienced an acute cardiovascular event or have homozygous or severe forms of heterozygous FH. In these cases, the decision to continue therapy during pregnancy should weigh the potential risks of discontinuation. Bempedoic acid, olezarsen, evinacumab, evolocumab and alirocumab, and inclisiran are options to consider just before and after pregnancy is completed. In conclusion, decisions regarding lipid-lowering therapy for pregnant patients should be personalized. Despite the challenges in designing and conducting studies in pregnant women, there is a strong need to establish the safety and efficacy of dyslipidaemia treatment during pregnancy.
几十年来,孕期血脂异常的治疗方法基本没有改变。该领域缺乏进展主要是因为我们缺乏针对现有疗法和新疗法的孕妇临床试验。虽然为非孕妇开发了众多新疗法,但孕期血脂异常治疗仍存在许多局限性。除药物治疗和仔细的临床评估外,启动行为改变以及孕前管理非常重要。在各种降脂药物中,胆汁酸螯合剂是唯一官方批准用于治疗孕期血脂异常的药物。如果依折麦布和非诺贝特的益处大于潜在风险,可以考虑使用。他汀类药物仍被视为禁忌,主要基于动物研究和人类病例报告。然而,最近的系统评价和荟萃分析以及关于孕妇家族性高胆固醇血症(FH)的数据表明,在某些特定情况下使用他汀类药物可能无害甚至有益。这对于心血管风险非常高的孕妇尤其相关,例如那些已经经历过急性心血管事件或患有纯合子或严重杂合子FH的孕妇。在这些情况下,孕期继续治疗的决定应权衡停药的潜在风险。在孕期即将结束前和结束后,可以考虑使用贝派地酸、olezarsen、evinacumab、evolocumab、alirocumab和inclisiran。总之,针对孕妇降脂治疗的决策应个性化。尽管在孕妇中设计和开展研究存在挑战,但迫切需要确定孕期血脂异常治疗的安全性和有效性。