Department of Internal Medicine, Mount Sinai Beth Israel, New York, NY.
Department of Critical Care Medicine, Department of Medicine, The Queen's Medical Center, Honolulu, HI.
Crit Care Explor. 2024 May 24;6(6):e1096. doi: 10.1097/CCE.0000000000001096. eCollection 2024 Jun 1.
Measurement of blood pressure taken from different anatomical sites, are often perceived as interchangeable, despite them representing different parts of the systemic circulation. We aimed to perform a systematic review and meta-analysis on blood pressure differences between central and peripheral arterial cannulation in critically ill patients.
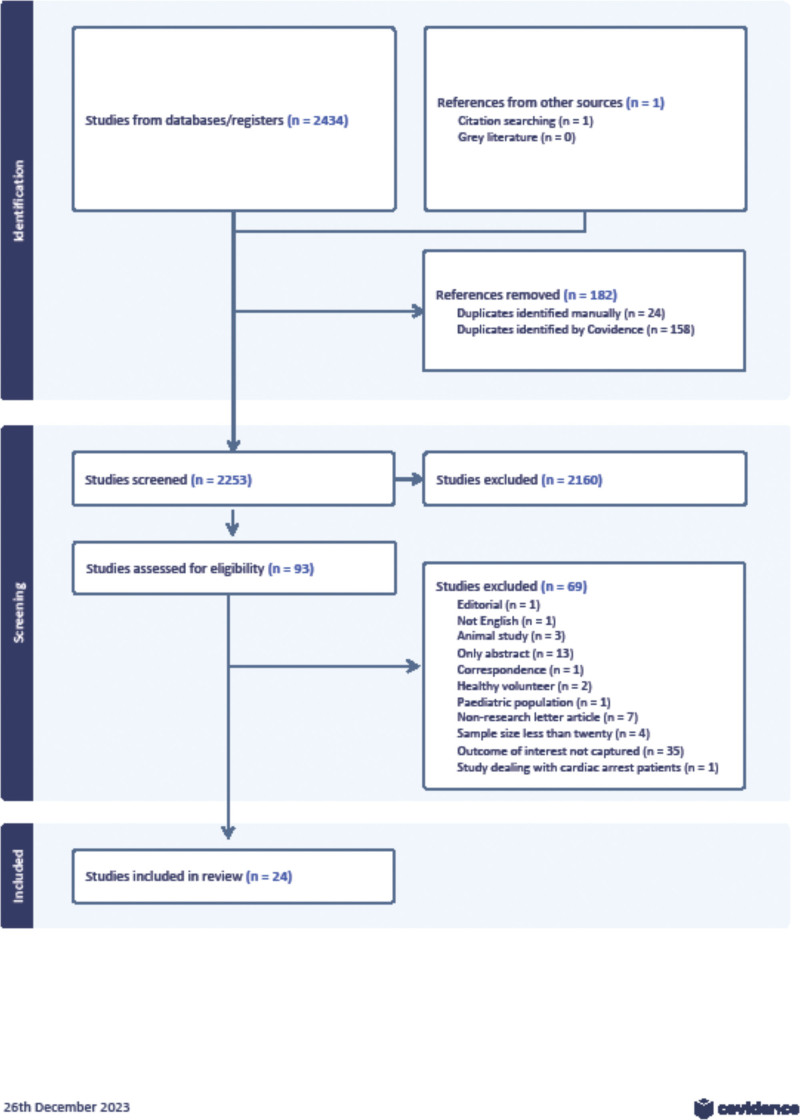
We searched MEDLINE, Cochrane Central Register of Controlled Trials, and Embase from inception to December 26, 2023, using Medical Subject Headings (MeSH) terms and keywords.
Observation study of adult patients in ICUs and operating rooms who underwent simultaneous central (femoral, axillary, or subclavian artery) and peripheral (radial, brachial, or dorsalis pedis artery) arterial catheter placement in ICUs and operating rooms.
We screened and extracted studies independently and in duplicate. We assessed risk of bias using the revised Quality Assessment for Studies of Diagnostic Accuracy tool.
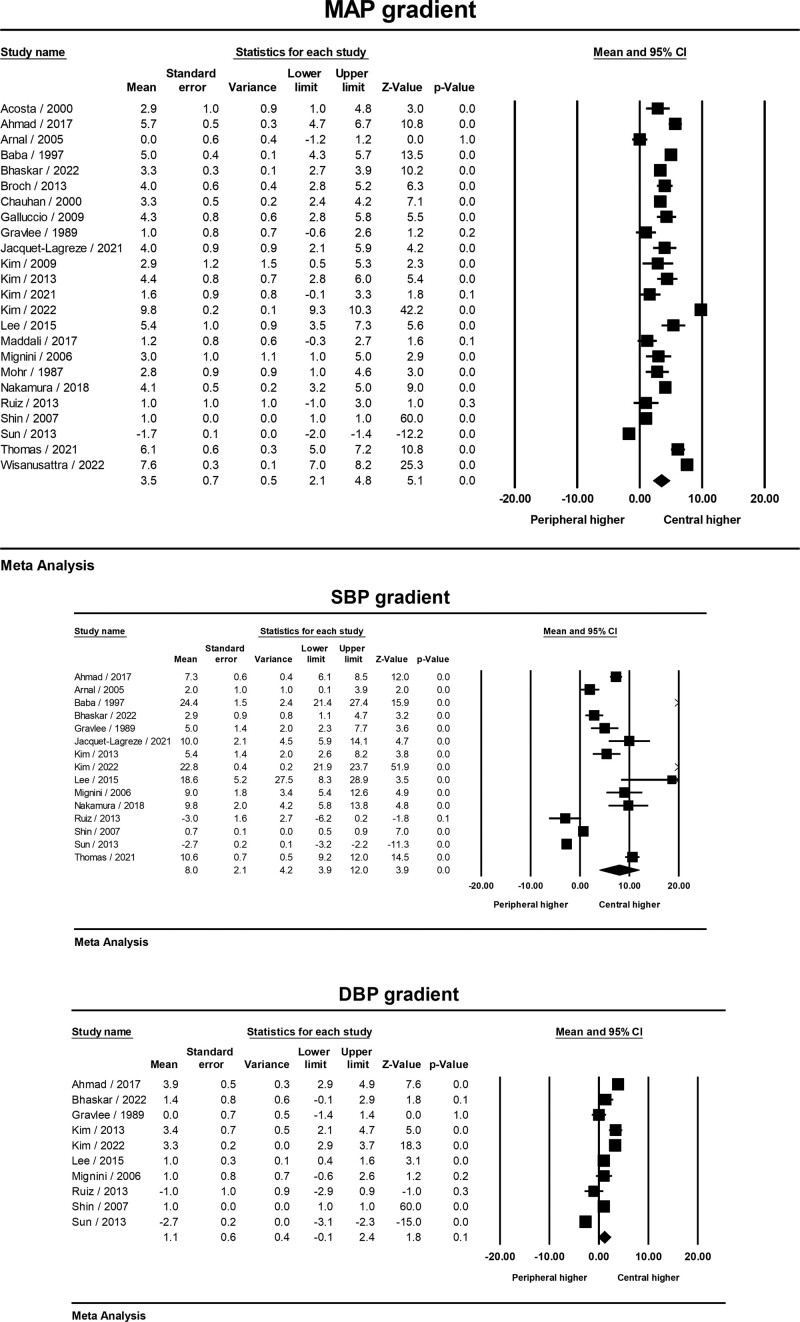
Twenty-four studies that enrolled 1598 patients in total were included. Central pressures (mean arterial pressure [MAP] and systolic blood pressure [SBP]) were found to be significantly higher than their peripheral counterparts, with mean gradients of 3.5 and 8.0 mm Hg, respectively. However, there was no statistically significant difference in central or peripheral diastolic blood pressure (DBP). Subgroup analysis further highlighted a higher MAP gradient during the on-cardiopulmonary bypass stage of cardiac surgery, reperfusion stage of liver transplant, and in nonsurgical critically ill patients. SBP or DBP gradient did not demonstrate any subgroup specific changes.
SBP and MAP obtained by central arterial cannulation were higher than peripheral arterial cannulation; however, clinical implication of a difference of 8.0 mm Hg in SBP and 3.5 mm Hg in MAP remains unclear. Our current clinical practices preferring peripheral arterial lines need not change.
尽管来自不同解剖部位的血压测量被认为是可互换的,但它们代表着全身循环的不同部分。我们旨在对危重病患者中心和外周动脉置管的血压差异进行系统评价和荟萃分析。
我们使用医学主题词(MeSH)术语和关键词,从 MEDLINE、Cochrane 对照试验中心注册库和 Embase 中搜索了从成立到 2023 年 12 月 26 日的文献。
对同时进行中心(股动脉、腋动脉或锁骨下动脉)和外周(桡动脉、肱动脉或足背动脉)动脉置管的 ICU 和手术室中的成年患者进行观察性研究。
我们独立并重复筛选和提取研究。我们使用修订后的诊断准确性研究质量评估工具评估偏倚风险。
共纳入 24 项研究,总计 1598 例患者。中心压(平均动脉压 [MAP] 和收缩压 [SBP])明显高于外周压,平均梯度分别为 3.5 和 8.0mmHg。然而,中心或外周舒张压(DBP)之间没有统计学差异。亚组分析进一步强调了在心脏手术体外循环阶段、肝移植再灌注阶段和非手术危重病患者中 MAP 梯度更高。SBP 或 DBP 梯度没有表现出任何亚组特异性变化。
中心动脉置管获得的 SBP 和 MAP 高于外周动脉置管;然而,SBP 差值 8.0mmHg 和 MAP 差值 3.5mmHg 的临床意义尚不清楚。我们目前的临床实践优先选择外周动脉线,无需改变。