Uveitis Service, Aravind Eye Hospital and PG Institute of Ophthalmology, Anna Nagar, Madurai, Tamil Nadu, India.
Department of Biostatistics, Aravind Eye Hospital and PG Institute of Ophthalmology, Anna Nagar, Madurai, Tamil Nadu, India.
Indian J Ophthalmol. 2024 Jun 1;72(6):869-877. doi: 10.4103/IJO.IJO_1376_23. Epub 2024 Mar 8.
Leptospirosis is a waterborne zoonotic disease prevalent in tropical regions, causing significant morbidity and mortality. It can involve any organ in its primary stage, and uveitis is its late complication. While advanced laboratory diagnosis is available only in tertiary care centers globally, a cost-effective bedside assessment of clinical signs and their scoring could offer a provisional diagnosis.
To analyze the diagnostic potential of demographic and clinical signs in a large cohort of serologically confirmed leptospiral uveitis patients.
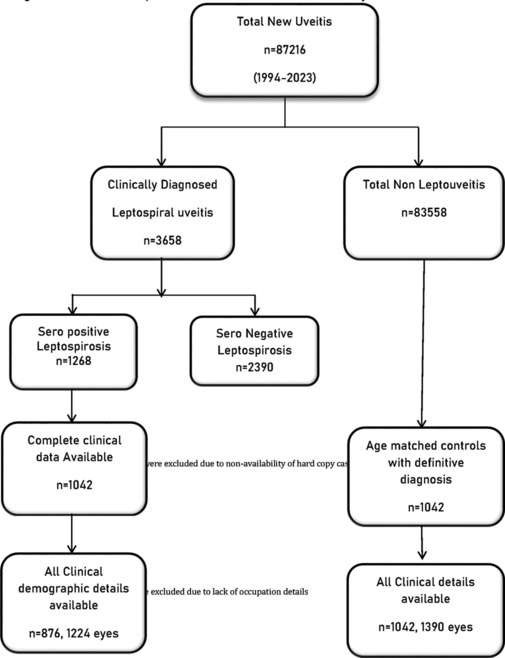
In this retrospective study, demographic and clinical parameters of 876 seropositive leptospiral uveitis patients and 1042 nonleptospiral uveitis controls were studied. Multivariable logistic regression analysis with bootstrap confidence interval (CI) characterized the diagnostic predictors. The performance of the model was evaluated using the area under the receiver operating curve (AUROC).
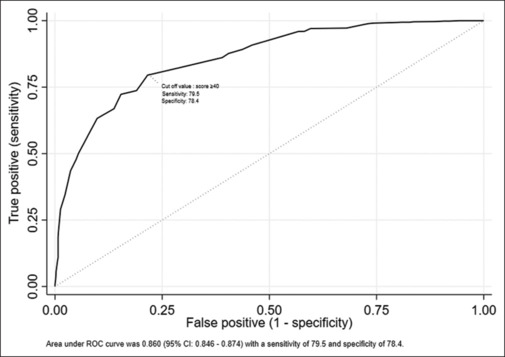
Presence of nongranulomatous uveitis (odds ratio [OR] = 6.9), hypopyon (OR = 4.6), vitreous infiltration with membranous opacities (OR = 4.3), bilateral involvement (OR = 4), panuveitis (OR = 3.3), vasculitis (OR = 1.9), disc hyperemia (OR = 1.6), absence of retinochoroiditis (OR = 15), and absence of cystoid macular edema (OR = 8.9) emerged as predictive parameters. The AUROC value was 0.86 with 95% CI of 0.846-0.874. At a cut-off score of 40, the sensitivity and specificity were 79.5 and 78.4, respectively.
The study demonstrates that ocular signs can serve as diagnostic predictors for leptospiral uveitis, enabling primary care ophthalmologists to make bedside diagnosis. This can be further confirmed by laboratory methods available at tertiary care centers.
钩端螺旋体病是一种流行于热带地区的水源性人畜共患疾病,可导致严重的发病率和死亡率。它在初期阶段可累及任何器官,而葡萄膜炎是其晚期并发症。虽然全球只有在三级护理中心才能进行先进的实验室诊断,但对临床体征及其评分进行经济有效的床边评估可能可以提供临时诊断。
分析大样本血清学确诊的钩端螺旋体性葡萄膜炎患者的人口统计学和临床体征的诊断潜力。
在这项回顾性研究中,研究了 876 例血清阳性钩端螺旋体性葡萄膜炎患者和 1042 例非钩端螺旋体性葡萄膜炎对照者的人口统计学和临床参数。采用具有 bootstrap 置信区间(CI)的多变量逻辑回归分析来确定诊断预测因素。使用接收者操作特征曲线(AUROC)下面积来评估模型的性能。
存在非肉芽肿性葡萄膜炎(优势比[OR] = 6.9)、前房积脓(OR = 4.6)、玻璃体浸润伴膜性混浊(OR = 4.3)、双侧受累(OR = 4)、全葡萄膜炎(OR = 3.3)、血管炎(OR = 1.9)、视盘充血(OR = 1.6)、无脉络膜视网膜炎(OR = 15)和无囊样黄斑水肿(OR = 8.9)是预测参数。AUROC 值为 0.86,95%CI 为 0.846-0.874。在截断评分 40 时,敏感性和特异性分别为 79.5%和 78.4%。
该研究表明,眼部体征可作为钩端螺旋体性葡萄膜炎的诊断预测因素,使初级保健眼科医生能够进行床边诊断。这可以通过三级护理中心提供的实验室方法进一步证实。