Alberta Research Centre for Health Evidence, Faculty of Medicine and Dentistry, University of Alberta, 11405 87 Avenue NW, Edmonton, Alberta, T6G 1C9, Canada.
Syst Rev. 2024 May 28;13(1):140. doi: 10.1186/s13643-024-02539-8.
Different guideline panels, and individuals, may make different decisions based in part on their preferences. Preferences for or against an intervention are viewed as a consequence of the relative importance people place on the expected or experienced health outcomes it incurs. These findings can then be considered as patient input when balancing effect estimates on benefits and harms reported by empirical evidence on the clinical effectiveness of screening programs. This systematic review update examined the relative importance placed by patients on the potential benefits and harms of mammography-based breast cancer screening to inform an update to the 2018 Canadian Task Force on Preventive Health Care's guideline on screening.
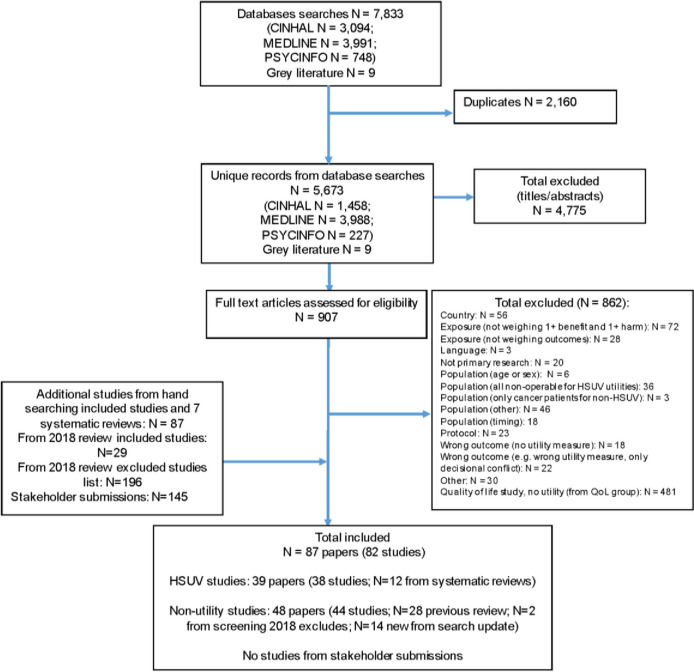
We screened all articles from our previous review (search December 2017) and updated our searches to June 19, 2023 in MEDLINE, PsycINFO, and CINAHL. We also screened grey literature, submissions by stakeholders, and reference lists. The target population was cisgender women and other adults assigned female at birth (including transgender men and nonbinary persons) aged ≥ 35 years and at average or moderately increased risk for breast cancer. Studies of patients with breast cancer were eligible for health-state utility data for relevant outcomes. We sought three types of data, directly through (i) disutilities of screening and curative treatment health states (measuring the impact of the outcome on one's health-related quality of life; utilities measured on a scale of 0 [death] to 1 [perfect health]), and (ii) other preference-based data, such as outcome trade-offs, and indirectly through (iii) the relative importance of benefits versus harms inferred from attitudes, intentions, and behaviors towards screening among patients provided with estimates of the magnitudes of benefit(s) and harms(s). For screening, we used machine learning as one of the reviewers after at least 50% of studies had been reviewed in duplicate by humans; full-text selection used independent review by two humans. Data extraction and risk of bias assessments used a single reviewer with verification. Our main analysis for utilities used data from utility-based health-related quality of life tools (e.g., EQ-5D) in patients; a disutility value of about 0.04 can be considered a minimally important value for the Canadian public. When suitable, we pooled utilities and explored heterogeneity. Disutilities were calculated for screening health states and between different treatment states. Non-utility data were grouped into categories, based on outcomes compared (e.g. for trade-off data), participant age, and our judgements of the net benefit of screening portrayed by the studies. Thereafter, we compared and contrasted findings while considering sample sizes, risk of bias, subgroup findings and data on knowledge scores, and created summary statements for each data set. Certainty assessments followed GRADE guidance for patient preferences and used consensus among at least two reviewers.
Eighty-two studies (38 on utilities) were included. The estimated disutilities were 0.07 for a positive screening result (moderate certainty), 0.03-0.04 for a false positive (FP; "additional testing" resolved as negative for cancer) (low certainty), and 0.08 for untreated screen-detected cancer (moderate certainty) or (low certainty) an interval cancer. At ≤12 months, disutilities of mastectomy (vs. breast-conserving therapy), chemotherapy (vs. none) (low certainty), and radiation therapy (vs. none) (moderate certainty) were 0.02-0.03, 0.02-0.04, and little-to-none, respectively, though in each case findings were somewhat limited in their applicability. Over the longer term, there was moderate certainty for little-to-no disutility from mastectomy versus breast-conserving surgery/lumpectomy with radiation and from radiation. There was moderate certainty that a majority (>50%) and possibly a large majority (>75%) of women probably accept up to six cases of overdiagnosis to prevent one breast-cancer death; there was some uncertainty because of an indication that overdiagnosis was not fully understood by participants in some cases. Low certainty evidence suggested that a large majority may accept that screening may reduce breast-cancer but not all-cause mortality, at least when presented with relatively high rates of breast-cancer mortality reductions (n = 2; 2 and 5 fewer per 1000 screened), and at least a majority accept that to prevent one breast-cancer death at least a few hundred patients will receive a FP result and 10-15 will have a FP resolved through biopsy. An upper limit for an acceptable number of FPs was not evaluated. When using data from studies assessing attitudes, intentions, and screening behaviors, across all age groups but most evident for women in their 40s, preferences reduced as the net benefit presented by study authors decreased in magnitude. In a relatively low net-benefit scenario, a majority of patients in their 40s may not weigh the benefits as greater than the harms from screening whereas for women in their 50s a large majority may prefer screening (low certainty evidence for both ages). There was moderate certainty that a large majority of women 50 years of age and 50 to 69 years of age, who have usually experienced screening, weigh the benefits as greater than the harms from screening in a high net-benefit scenario. A large majority of patients aged 70-71 years who have recently screened probably think the benefits outweigh the harms of continuing to screen. A majority of women in their mid-70s to early 80s may prefer to continue screening.
Evidence across a range of data sources on how informed patients value the potential outcomes from breast-cancer screening will be useful during decision-making for recommendations. The evidence suggests that all of the outcomes examined have importance to women of any age, that there is at least some and possibly substantial (among those in their 40s) variability across and within age groups about the acceptable magnitude of effects across outcomes, and that provision of easily understandable information on the likelihood of the outcomes may be necessary to enable informed decision making. Although studies came from a wide range of countries, there were limited data from Canada and about whether findings applied well across an ethnographically and socioeconomically diverse population.
Protocol available at Open Science Framework https://osf.io/xngsu/ .
不同的指南小组和个人可能会根据部分偏好做出不同的决策。对干预措施的偏好或反对被视为人们对其引发的预期或经历的健康结果的相对重要性的结果。当根据有关筛查计划临床有效性的经验证据报告的益处和危害的平衡效应估计值来考虑这些发现时,这些发现可以被视为患者输入。本系统评价更新检查了患者对基于乳房 X 光筛查的乳腺癌筛查的潜在益处和危害的相对重视程度,以告知 2018 年加拿大预防保健工作组关于筛查的指南更新。
我们筛查了我们之前的综述(2017 年 12 月搜索)中的所有文章,并将我们的搜索更新至 2023 年 6 月 19 日,在 MEDLINE、PsycINFO 和 CINAHL 中进行了更新。我们还筛查了灰色文献、利益相关者的提交和参考文献列表。目标人群是年龄在 35 岁及以上、平均或中度增加乳腺癌风险的顺性别女性和其他出生时被指定为女性的成年人(包括跨性别男性和非二进制人)。患有乳腺癌的患者的研究符合相关结果的健康状态效用数据的入选标准。我们寻求三种类型的数据,直接通过(i)筛查和治疗性治疗健康状态的不良效用(衡量结果对一个人健康相关生活质量的影响;效用在 0 [死亡] 到 1 [完美健康] 的范围内测量),以及(ii)其他基于偏好的数据,如结果权衡,以及(iii)通过向患者提供对益处(s)和危害(s)的估计值的态度、意图和行为对筛查的相对重视程度推断出的益处与危害之间的相对重要性。对于筛查,我们在至少 50%的研究由人类进行了重复审查后,使用机器学习作为其中一位审稿人;全文选择由两名人类进行独立审查。数据提取和偏倚风险评估使用单一审查员进行,验证后进行。我们对效用的主要分析使用了来自患者使用的基于效用的健康相关生活质量工具(例如,EQ-5D)的数据;大约 0.04 的不良效用值可以被认为是加拿大公众的最小重要值。在合适的情况下,我们会对效用进行汇总,并探讨异质性。不良效用值是为筛查健康状态和不同治疗状态之间计算的。非效用数据根据比较的结果(例如,用于权衡数据)、参与者年龄以及我们对研究描绘的筛查收益的净收益的判断分组。此后,我们在考虑样本量、偏倚风险、亚组发现和有关知识得分的数据的同时进行了比较和对比,并为每个数据集创建了总结陈述。基于患者偏好的 GRADE 指南对确定性评估进行了使用,共识至少需要两名审稿人达成。
共纳入 82 项研究(38 项涉及效用)。估计的不良效用为阳性筛查结果为 0.07(中度确定性),假阳性(“额外检测”结果为阴性而无癌症)为 0.03-0.04(低确定性),未治疗的筛检发现的癌症为 0.08(中度确定性)或(低确定性)间隔期癌症。在 12 个月内,乳房切除术(与保乳治疗相比)、化疗(与无化疗相比)(低确定性)和放射治疗(与无放射治疗相比)(中度确定性)的不良效用分别为 0.02-0.03、0.02-0.04 和几乎没有。然而,在每种情况下,发现的适用性都有些有限。在较长的时间内,有中度确定性的是,与乳房切除术/保乳术加放疗相比,大多数(>50%)甚至可能是大多数(>75%)女性可能接受多达 6 例过度诊断以预防 1 例乳腺癌死亡;有一些不确定性,因为这表明在某些情况下,参与者没有完全理解过度诊断。低确定性证据表明,大多数人可能会接受筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会接受,筛查可能会降低乳腺癌死亡率,但不能降低所有原因死亡率,至少当呈现出相对较高的乳腺癌死亡率降低率(n = 2;每 1000 名筛查者减少 2 或 5 例)时,并且至少大多数人接受的是大多数人可能会