Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University, Shandong Academy of Medical Sciences, Jinan, China.
Department of Intensive Care Unit, Shandong Cancer Hospital and Institute, Shandong First Medical University, Shandong Academy of Medical Sciences, 440 Jiyan Road, Jinan, 250117, Shandong, China.
Radiat Oncol. 2024 May 30;19(1):67. doi: 10.1186/s13014-024-02458-x.
First-line chemotherapy combined with bevacizumab is one of the standard treatment modes for patients with advanced non-small cell lung cancer (NSCLC). Thoracic radiotherapy (TRT) can provide significant local control and survival benefits to patients during the treatment of advanced NSCLC. However, the safety of adding TRT has always been controversial, especially because of the occurrence of radiation pneumonia (RP) during bevacizumab treatment. Therefore, in this study, we used an expanded sample size to evaluate the incidence of RP when using bevacizumab in combination with TRT.
Using an institutional query system, all medical records of patients with NSCLC who received TRT during first-line chemotherapy combined with bevacizumab from 2017 to 2020 at Shandong Cancer Hospital and Institute were reviewed. RP was diagnosed via computed tomography and was classified according to the RTOG toxicity scoring system. The risk factors for RP were identified using univariate and multivariate analyses. The Kaplan-Meier method was used to calculate progression-free survival (PFS) and overall survival (OS).
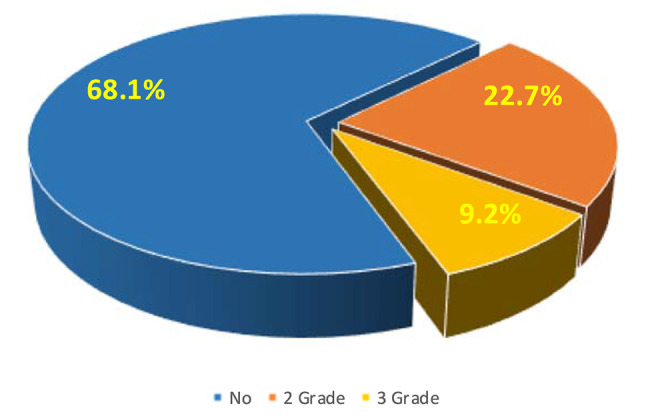
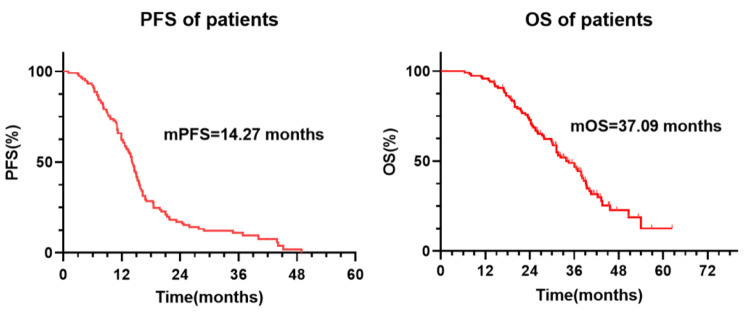
Ultimately, 119 patients were included. Thirty-eight (31.9%) patients developed Grade ≥ 2 RP, of whom 27 (68.1%) had Grade 2 RP and 11 (9.2%) had Grade 3 RP. No patients developed Grade 4 or 5 RP. The median time for RP occurrence was 2.7 months (range 1.2-5.4 months). In univariate analysis, male, age, KPS score, V > 16.9%, V > 33.6%, PTV (planning target volume)-dose > 57.2 Gy, and PTV-volume > 183.85 cm were correlated with the occurrence of RP. In multivariate analysis, male, V > 16.9%, and PTV-volume > 183.85 cm were identified as independent predictors of RP occurrence. The mPFS of all patients was 14.27 (95% CI, 13.1-16.1) months. The one-year and two-year PFS rates were 64.9% and 20.1%, respectively. The mOS of all patients was 37.09 (95% CI, 33.8-42.0) months. The one-year survival rate of all patients was 95%, and the two-year survival rate was 71.4%.
The incidence of Grade ≥ 2 RP in NSCLC patients who received both bevacizumab and TRT was 31.9%. Restricting factors such as V and PTV will help reduce the risk of RP in these patients. For patients who receive both bevacizumab and TRT, caution should be exercised when increasing TRT, and treatment strategies should be optimized to reduce the incidence of RP.
一线化疗联合贝伐珠单抗是治疗晚期非小细胞肺癌(NSCLC)患者的标准治疗模式之一。胸部放疗(TRT)在治疗晚期 NSCLC 期间可为患者提供显著的局部控制和生存获益。然而,添加 TRT 的安全性一直存在争议,特别是因为在贝伐珠单抗治疗期间发生放射性肺炎(RP)。因此,在这项研究中,我们使用扩大的样本量来评估在贝伐珠单抗联合 TRT 治疗时 RP 的发生率。
使用机构查询系统,回顾了 2017 年至 2020 年在山东省肿瘤医院和研究所接受一线化疗联合贝伐珠单抗治疗的 NSCLC 患者的所有病历,这些患者在接受 TRT 治疗。通过计算机断层扫描诊断 RP,并根据 RTOG 毒性评分系统进行分类。使用单因素和多因素分析确定 RP 的危险因素。使用 Kaplan-Meier 方法计算无进展生存期(PFS)和总生存期(OS)。
最终纳入 119 例患者。38 例(31.9%)患者发生≥2 级 RP,其中 27 例(68.1%)为 2 级 RP,11 例(9.2%)为 3 级 RP。无 4 级或 5 级 RP 病例。RP 发生的中位时间为 2.7 个月(范围 1.2-5.4 个月)。单因素分析中,男性、年龄、KPS 评分、V>16.9%、V>33.6%、PTV(计划靶区)剂量>57.2 Gy 和 PTV 体积>183.85 cm 与 RP 发生相关。多因素分析中,男性、V>16.9%和 PTV 体积>183.85 cm 被确定为 RP 发生的独立预测因子。所有患者的 mPFS 为 14.27(95%CI,13.1-16.1)个月。一年和两年的 PFS 率分别为 64.9%和 20.1%。所有患者的 mOS 为 37.09(95%CI,33.8-42.0)个月。所有患者的 1 年生存率为 95%,2 年生存率为 71.4%。
接受贝伐珠单抗和 TRT 联合治疗的 NSCLC 患者中,≥2 级 RP 的发生率为 31.9%。限制 V 和 PTV 等因素将有助于降低这些患者发生 RP 的风险。对于接受贝伐珠单抗和 TRT 联合治疗的患者,在增加 TRT 时应谨慎,并优化治疗策略以降低 RP 的发生率。