UMC Utrecht Brain Center, Department of Neurology and Neurosurgery, University Medical Center Utrecht, Utrecht, The Netherlands.
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
PLoS One. 2024 May 31;19(5):e0303868. doi: 10.1371/journal.pone.0303868. eCollection 2024.
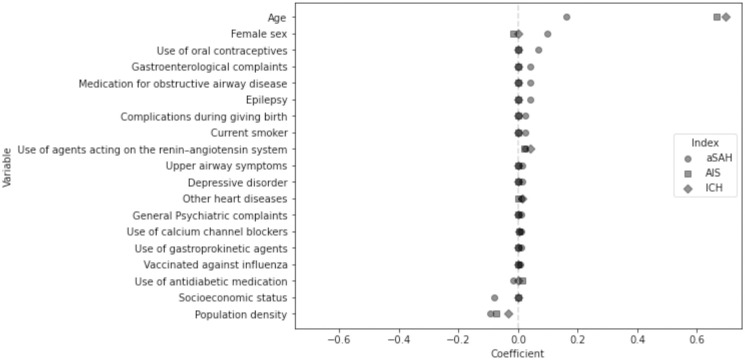
Aneurysmal subarachnoid hemorrhage (aSAH) can be prevented by early detection and treatment of intracranial aneurysms in high-risk individuals. We investigated whether individuals at high risk of aSAH in the general population can be identified by developing an aSAH prediction model with electronic health records (EHR) data. To assess the aSAH model's relative performance, we additionally developed prediction models for acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH) and compared the discriminative performance of the models. We included individuals aged ≥35 years without history of stroke from a Dutch routine care database (years 2007-2020) and defined outcomes aSAH, AIS and ICH using International Classification of Diseases (ICD) codes. Potential predictors included sociodemographic data, diagnoses, medications, and blood measurements. We cross-validated a Cox proportional hazards model with an elastic net penalty on derivation cohorts and reported the c-statistic and 10-year calibration on validation cohorts. We examined 1,040,855 individuals (mean age 54.6 years, 50.9% women) for a total of 10,173,170 person-years (median 11 years). 17,465 stroke events occurred during follow-up: 723 aSAH, 14,659 AIS, and 2,083 ICH. The aSAH model's c-statistic was 0.61 (95%CI 0.57-0.65), which was lower than the c-statistic of the AIS (0.77, 95%CI 0.77-0.78) and ICH models (0.77, 95%CI 0.75-0.78). All models were well-calibrated. The aSAH model identified 19 predictors, of which the 10 strongest included age, female sex, population density, socioeconomic status, oral contraceptive use, gastroenterological complaints, obstructive airway medication, epilepsy, childbirth complications, and smoking. Discriminative performance of the aSAH prediction model was moderate, while it was good for the AIS and ICH models. We conclude that it is currently not feasible to accurately identify individuals at increased risk for aSAH using EHR data.
颅内动脉瘤破裂是蛛网膜下腔出血(aSAH)的主要原因。通过对高危人群的早期发现和治疗,可以预防颅内动脉瘤破裂。我们研究了是否可以通过电子健康记录(EHR)数据建立 aSAH 预测模型来识别一般人群中的高危个体。为了评估 aSAH 模型的相对性能,我们还为急性缺血性中风(AIS)和脑出血(ICH)开发了预测模型,并比较了模型的判别性能。我们纳入了来自荷兰常规护理数据库(2007-2020 年)的年龄≥35 岁且无中风史的个体,并使用国际疾病分类(ICD)代码定义了 aSAH、AIS 和 ICH 结局。潜在的预测因素包括社会人口统计学数据、诊断、药物和血液测量值。我们在推导队列中使用具有弹性网惩罚的 Cox 比例风险模型进行了交叉验证,并在验证队列中报告了 c 统计量和 10 年校准值。我们对 1040855 名个体(平均年龄 54.6 岁,50.9%为女性)进行了随访,共随访 10173170 人年(中位数 11 年)。随访期间共发生 17465 例中风事件:723 例 aSAH,14659 例 AIS 和 2083 例 ICH。aSAH 模型的 c 统计量为 0.61(95%CI 0.57-0.65),低于 AIS(0.77,95%CI 0.77-0.78)和 ICH 模型(0.77,95%CI 0.75-0.78)的 c 统计量。所有模型的校准效果都很好。aSAH 模型确定了 19 个预测因素,其中最强的 10 个因素包括年龄、女性、人口密度、社会经济地位、口服避孕药使用、胃肠道投诉、气道阻塞药物、癫痫、分娩并发症和吸烟。aSAH 预测模型的判别性能为中等,而 AIS 和 ICH 模型的判别性能较好。我们的结论是,目前使用 EHR 数据准确识别 aSAH 风险增加的个体是不可行的。