van Weringh Geke, van Koolwijk Leonieke, de Haan Lieuwe, Touw Daan J, de Koning Mariken B
Groningen Research Institute of Pharmacy, University of Groningen, Antonius Deusinglaan 1, Groningen 9713 AV, The Netherlands.
Department of Clinical Pharmacy, OLVG Hospital, Amsterdam, The Netherlands.
Ther Adv Psychopharmacol. 2024 May 31;14:20451253241255487. doi: 10.1177/20451253241255487. eCollection 2024.
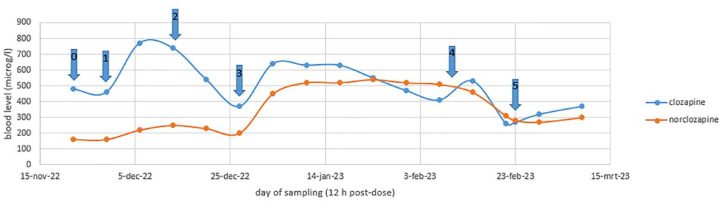
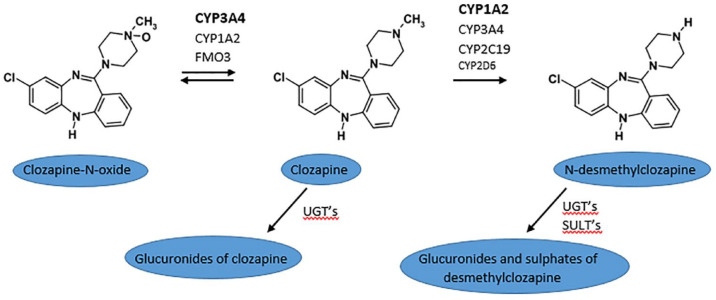
This case report examines the possible correlation between the clozapine/norclozapine ratio and the occurrence of constipation and paralytic ileus. We present the case of a 42-year-old patient diagnosed with schizoaffective disorder undergoing clozapine therapy. Despite intensive treatment with clozapine, haloperidol, valproic acid and biweekly electroconvulsive therapy sessions for over a year, florid psychotic symptoms and fluctuating mood swings persisted. Therefore, valproic acid was replaced by carbamazepine, a potent inducer of several CYP450-enzymes. To maintain clozapine plasma levels, fluvoxamine, a CYP1A2-inhibitor, was introduced at a dose of 25 mg before this switch. After addition of carbamazepine, there was a significant decline in clozapine levels, necessitating an increase in fluvoxamine dosage to 50 mg. Five weeks later the patient was admitted to a general hospital with a diagnosis of paralytic ileus. Treatment with enemas proved effective. Drug concentration analysis revealed a 2.5-fold increase in norclozapine levels in the weeks preceding hospital admission, resulting in an inverted clozapine/norclozapine ratio. Treatment with clozapine, carbamazepine and fluvoxamine was continued as the patient demonstrated clinical improvement on carbamazepine. Concurrently, an intensive laxative regimen was initiated. Two weeks later, the patient was readmitted to the general hospital due to suspected paralytic ileus and faecal vomiting, once again displaying an inverted clozapine/norclozapine ratio. We discuss potential mechanisms contributing to the occurrence of the paralytic ileus in this patient, including the antagonism of muscarinic M3 receptors by both clozapine and norclozapine, as well as the agonism of delta-opioid receptors by norclozapine. This case highlights the potential significance of both the clozapine/norclozapine ratio and absolute norclozapine levels as risk factors for constipation and paralytic ileus in patients on clozapine therapy.
本病例报告探讨了氯氮平/去甲氯氮平比值与便秘及麻痹性肠梗阻发生之间的可能关联。我们报告一例42岁诊断为分裂情感性障碍且正在接受氯氮平治疗的患者。尽管使用氯氮平、氟哌啶醇、丙戊酸进行了强化治疗,并每两周进行一次电休克治疗,持续一年多,但明显的精神病性症状和波动的情绪 swings仍持续存在。因此,丙戊酸被卡马西平取代,卡马西平是几种CYP450酶的强效诱导剂。为维持氯氮平血浆水平,在换药前引入了剂量为25mg的CYP1A2抑制剂氟伏沙明。添加卡马西平后,氯氮平水平显著下降,因此需要将氟伏沙明剂量增加至50mg。五周后,该患者因诊断为麻痹性肠梗阻入住综合医院。灌肠治疗证明有效。药物浓度分析显示,入院前几周去甲氯氮平水平增加了2.5倍,导致氯氮平/去甲氯氮平比值倒置。由于患者在卡马西平治疗下临床症状改善,继续使用氯氮平、卡马西平和氟伏沙明治疗。同时,启动了强化泻药方案。两周后,患者因疑似麻痹性肠梗阻和粪便呕吐再次入住综合医院,氯氮平/去甲氯氮平比值再次倒置。我们讨论了导致该患者发生麻痹性肠梗阻的潜在机制,包括氯氮平和去甲氯氮平对毒蕈碱M3受体的拮抗作用,以及去甲氯氮平对δ阿片受体的激动作用。本病例突出了氯氮平/去甲氯氮平比值和去甲氯氮平绝对水平作为氯氮平治疗患者便秘和麻痹性肠梗阻危险因素的潜在重要性。