From the Department of Laboratory Medicine (K.B., E.R.B., E.A.J.W., C.E.T.) and Alzheimer Center Amsterdam (A.A.J.M.U., A.W.L.), Amsterdam UMC, the Netherlands; Department of Quality and Health Technology (M.C.G.), University of Stavanger; The Norwegian Centre for Movement Disorders (M.C.G.) and the Centre for Age-Related Medicine (M.C.G., N.J.A., D.A.), Stavanger University Hospital, Norway; Department of Psychiatry and Neurochemistry (N.J.A., H.Z.), the Sahlgrenska Academy at the University of Gothenburg, Mölndal, Sweden; Department of Old Age Psychiatry (N.J.A., D.A.), King's College London, United Kingdom; Clinical Neurochemistry Laboratory (H.Z.), Sahlgrenska University Hospital, Mölndal, Sweden; Department of Neurodegenerative Disease (H.Z.), UCL Institute of Neurology; UK Dementia Research Institute at UCL (H.Z.), London, United Kingdom; Hong Kong Center for Neurodegenerative Diseases (H.Z.), Hong Kong, China; Wisconsin Alzheimer's Disease Research Center (H.Z.), University of Wisconsin School of Medicine and Public Health, Madison; Neurology Unit (A.P.), Department of Clinical and Experimental Sciences, University of Brescia, Italy; Department of Medicine and Aging Sciences (L.B.), University G. d'Annunzio of Chieti-Pescara, Chieti, Italy; Department of Neurology (B.M.), University Medical Center Göttingen; Paracelsus-Elena-Klinik (B.M., S.S.), Germany; Department of Neurosciences (R.V., K.P.), KU Leuven, Belgium; Department of Neurology and Medical Faculty (M.G.K.), University Medical Center Ljubljana, Slovenia; Department of Neurobiology (M.G.K.), Karolinska Institutet, Huddinge, Sweden; Université de Paris Cité (C.P.), Centre de Neurologie Cognitive, Paris; Laboratory of Biochemistry and Molecular Biology (O.B.), University Hospital of Strasbourg; University of Strasbourg and CNRS (O.B., B.C.); Memory Resource and Research Centre (B.C.), University Hospital of Strasbourg, France; Department of Neurology (E.A.J.W.), Multiple Sclerosis Center; Research Center for Clinical Neuroimmunology and Neuroscience Basel (E.A.J.W.); and Departments of Biomedicine and Clinical Research (E.A.J.W.), University Hospital Basel and University of Basel, Switzerland.
Neurology. 2024 Jun 25;102(12):e209418. doi: 10.1212/WNL.0000000000209418. Epub 2024 Jun 3.
Plasma β-amyloid-1-42/1-40 (Aβ42/40), phosphorylated-tau (P-tau), glial fibrillary acidic protein (GFAP), and neurofilament light (NfL) have been widely examined in Alzheimer disease (AD), but little is known about their reflection of copathologies, clinical importance, and predictive value in dementia with Lewy bodies (DLB). We aimed to evaluate associations of these biomarkers with CSF amyloid, cognition, and core features in DLB.
This cross-sectional multicenter cohort study with prospective component included individuals with DLB, AD, and healthy controls (HCs), recruited from 2002 to 2020 with an annual follow-up of up to 5 years, from the European-Dementia With Lewy Bodies consortium. Plasma biomarkers were measured by single-molecule array (Neurology 4-Plex E kit). Amyloid status was determined by CSF Aβ42 concentrations, and cognition was assessed by Mini-Mental State Examination (MMSE). Biomarker differences across groups, associations with amyloid status, and clinical core features were assessed by analysis of covariance. Associations with cognitive impairment and decline were assessed by linear regression and linear mixed-effects models.
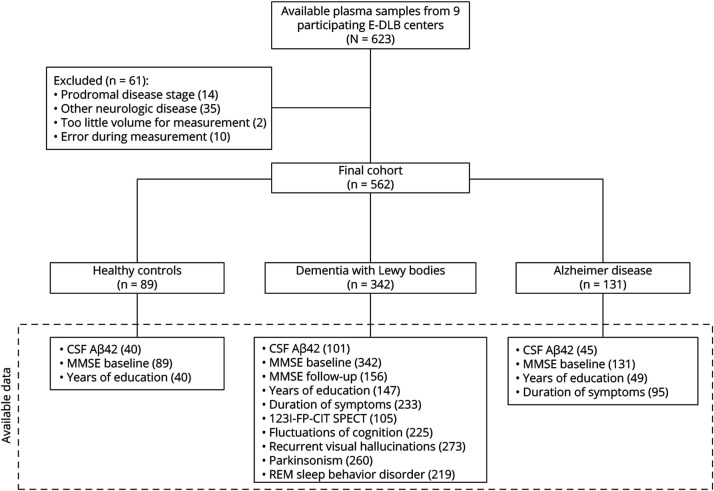
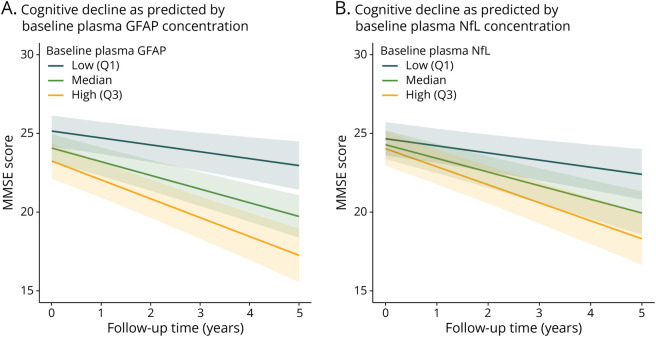
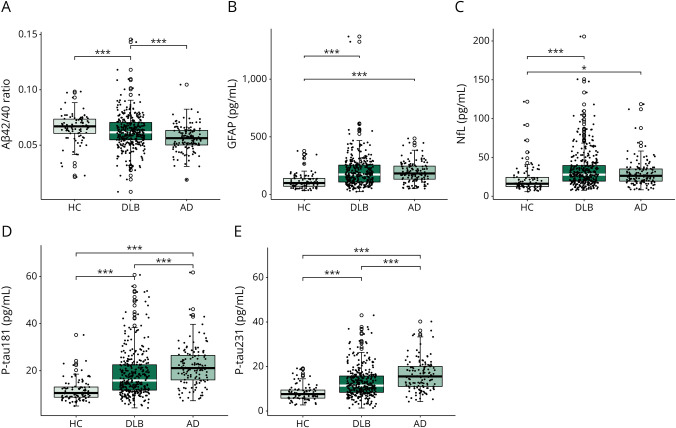
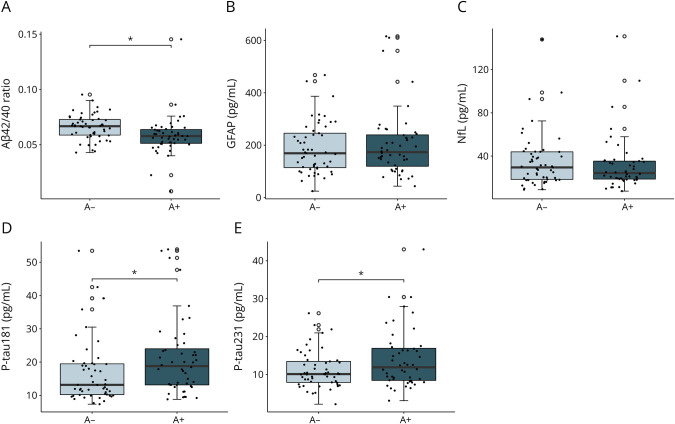
In our cohort consisting of 562 individuals (HC n = 89, DLB n = 342, AD n = 131; 250 women [44.5%], mean [SD] age of 71 [8] years), sex distribution did not differ between groups. Patients with DLB were significantly older, and had less years of education and worse baseline cognition than HC, but not AD. DLB participants stratified for amyloid status differed significantly in plasma Aβ42/40 ratio (decreased in amyloid abnormal: β = -0.008, 95% CI -0.016 to -0.0003, = 0.01) and P-tau (increased in amyloid abnormal, P-tau181: β = 0.246, 95% CI 0.011-0.481; P-tau231: β = 0.227, 95% CI 0.035-0.419, both < 0.05), but not in GFAP (β = 0.068, 95% CI -0.018 to 0.153, = 0.119), and NfL (β = 0.004, 95% CI -0.087 to 0.096, = 0.923) concentrations. Higher baseline GFAP, NfL, and P-tau concentrations were associated with lower MMSE scores in DLB, and GFAP and NfL were associated with a faster cognitive decline (GFAP: annual change of -2.11 MMSE points, 95% CI -2.88 to -1.35 MMSE points, < 0.001; NfL: annual change of -2.13 MMSE points, 95% CI -2.97 to -1.29 MMSE points, < 0.001). DLB participants with parkinsonism had higher concentrations of NfL (β = 0.08, 95% CI 0.02-0.14, = 0.006) than those without.
Our study suggests a possible utility of plasma Aβ42/40, P-tau181, and P-tau231 as a noninvasive biomarkers to assess amyloid copathology in DLB, and plasma GFAP and NfL as monitoring biomarkers for cognitive symptoms in DLB.
β-淀粉样蛋白 1-42/1-40(Aβ42/40)、磷酸化 tau(P-tau)、神经胶质纤维酸性蛋白(GFAP)和神经丝轻链(NfL)已广泛应用于阿尔茨海默病(AD)的研究,但关于其在路易体痴呆症(DLB)中的共病、临床重要性和预测价值的了解甚少。我们旨在评估这些生物标志物与脑脊液淀粉样蛋白、认知和 DLB 核心特征的相关性。
这是一项多中心横断面队列研究,前瞻性部分纳入了 2002 年至 2020 年期间从欧洲路易体痴呆症协会招募的 DLB、AD 和健康对照组(HC)患者,每年进行一次随访,最长可达 5 年。通过单分子阵列(Neurology 4-Plex E 试剂盒)测量血浆生物标志物。通过 CSF Aβ42 浓度确定淀粉样蛋白状态,通过 Mini-Mental State Examination(MMSE)评估认知。通过协方差分析评估各组之间的生物标志物差异、与淀粉样蛋白状态的相关性以及临床核心特征。通过线性回归和线性混合效应模型评估与认知障碍和认知下降的相关性。
在我们的队列中包括 562 名患者(HC 组 n = 89,DLB 组 n = 342,AD 组 n = 131;250 名女性[44.5%],平均[SD]年龄 71 [8] 岁),各组之间的性别分布无差异。DLB 患者年龄较大,受教育年限较短,基线认知能力较差,但与 AD 患者不同。根据淀粉样蛋白状态分层的 DLB 患者在血浆 Aβ42/40 比值(异常淀粉样蛋白降低:β=-0.008,95%CI-0.016 至-0.0003, = 0.01)和 P-tau(异常淀粉样蛋白增加:P-tau181:β=0.246,95%CI 0.011 至 0.481;P-tau231:β=0.227,95%CI 0.035 至 0.419,均 < 0.05)方面差异显著,但 GFAP(β=0.068,95%CI-0.018 至 0.153, = 0.119)和 NfL(β=0.004,95%CI-0.087 至 0.096, = 0.923)浓度则没有差异。DLB 患者基线 GFAP、NfL 和 P-tau 浓度较高与 MMSE 评分较低相关,而 GFAP 和 NfL 与认知下降较快相关(GFAP:每年 MMSE 评分下降 2.11 分,95%CI-2.88 至-1.35 分, < 0.001;NfL:每年 MMSE 评分下降 2.13 分,95%CI-2.97 至-1.29 分, < 0.001)。有帕金森病的 DLB 患者 NfL 浓度较高(β=0.08,95%CI 0.02 至 0.14, = 0.006)。
我们的研究表明,血浆 Aβ42/40、P-tau181 和 P-tau231 可能作为一种非侵入性生物标志物用于评估 DLB 中的淀粉样蛋白共病,而血浆 GFAP 和 NfL 则可用作 DLB 认知症状的监测生物标志物。