Barzilai Ori, Sahgal Arjun, Rhines Laurence D, Versteeg Anne L, Sciubba Daniel M, Lazary Aron, Weber Michael H, Schuster James M, Boriani Stefano, Bettegowda Chetan, Arnold Paul M, Clarke Michelle J, Laufer Ilya, Fehlings Michael G, Gokaslan Ziya L, Fisher Charles G
Department of Neurosurgery, Memorial Sloan Kettering Cancer Center, New York , New York , USA.
Department of Radiation Oncology, Sunnybrook Health Sciences Centre, University of Toronto, Toronto , Ontario , Canada.
Neurosurgery. 2024 Nov 1;95(5):1148-1157. doi: 10.1227/neu.0000000000002989. Epub 2024 Jun 4.
The palliative impact of spine surgery for metastatic disease is evolving with improvements in surgical technique and multidisciplinary cancer care. The goal of this study was to prospectively evaluate long-term clinical outcomes including health-related quality-of-life (HRQOL) measures, using spine cancer-specific patient-reported-outcome (PRO) measures, in patients with symptomatic spinal metastases who underwent surgical management.
The Epidemiology, Process, and Outcomes of Spine Oncology (EPOSO, ClinicalTrials.gov identifier: NCT01825161) trial is a prospective-observational cohort study that included 10 specialist centers in North America and Europe. Patients aged 18 to 75 years who underwent surgery for spinal metastases were included. Prospective assessments included both spine tumor-specific and generic PRO tools which were collected for a minimum of 2 years post-treatment or until death.
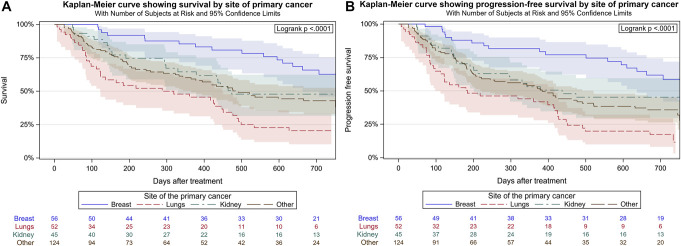
Two hundred and eighty patients (51.8% female, mean age 57.9 years) were included. At presentation, the mean Charlson Comorbidity Index was 6.0, 35.7% had neurological deficits as defined by the American Spinal Cord Injury Association scores, 47.2% had high-grade epidural spinal cord compression (2-3), and 89.6% had impending or frank instability as measured by a Spinal Instability Neoplastic Score of ≥7. The most common primary tumor sites were breast (20.2%), lung (18.8%), kidney (16.2%), and prostate (6.5%). The median overall survival postsurgery was 501 days, and the 2-year progression-free-survival rate was 38.4%. Compared with baseline, significant and durable improvements in HRQOL were observed at the 6-week, 12-week, 26-week, 1-year, and 2-year follow-up assessments from a battery of PRO questionnaires including the spine cancer-specific, validated, Spine Oncology Study Group Outcomes Questionnaire v2.0, the Short Form 36 version 2, EuroQol-5 Dimension (3L), and pain numerical rating scale score.
Multi-institutional, prospective-outcomes data confirm that surgical decompression and/or stabilization provides meaningful and durable improvements in multiple HRQOL domains, including spine-specific outcomes based on the Spine Oncology Study Group Outcomes Questionnaire v2.0, for patients with metastatic spine disease.
随着手术技术和多学科癌症治疗的改善,脊柱手术对转移性疾病的姑息治疗作用也在不断发展。本研究的目的是使用脊柱癌特异性患者报告结局(PRO)指标,对接受手术治疗的有症状脊柱转移瘤患者的长期临床结局进行前瞻性评估,包括健康相关生活质量(HRQOL)指标。
脊柱肿瘤学的流行病学、过程与结局(EPOSO,ClinicalTrials.gov标识符:NCT01825161)试验是一项前瞻性观察队列研究,纳入了北美和欧洲的10个专科中心。纳入年龄在18至75岁之间接受脊柱转移瘤手术的患者。前瞻性评估包括脊柱肿瘤特异性和通用的PRO工具,这些工具在治疗后至少收集2年或直至死亡。
共纳入280例患者(女性占51.8%,平均年龄57.9岁)。就诊时,平均查尔森合并症指数为6.0,35.7%的患者根据美国脊髓损伤协会评分存在神经功能缺损,47.2%的患者存在高级别硬膜外脊髓压迫(2 - 3级),89.6%的患者根据脊髓不稳定肿瘤评分≥7提示即将发生或已存在明显不稳定。最常见的原发肿瘤部位是乳腺(20.2%)、肺(18.8%)、肾(16.2%)和前列腺(6.5%)。术后中位总生存期为501天,2年无进展生存率为38.4%。与基线相比,在包括脊柱癌特异性、经过验证的脊柱肿瘤学研究组结局问卷v2.0、简短健康调查问卷第2版、欧洲五维健康量表(3L)和疼痛数字评分量表评分在内的一系列PRO问卷的6周、12周、26周、1年和2年随访评估中,观察到HRQOL有显著且持久的改善。
多机构前瞻性结局数据证实,对于转移性脊柱疾病患者,手术减压和/或稳定化在多个HRQOL领域提供了有意义且持久的改善,包括基于脊柱肿瘤学研究组结局问卷v2.0的脊柱特异性结局。