Department of Community Medicine, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka.
Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka.
BMC Prim Care. 2024 Jun 6;25(1):200. doi: 10.1186/s12875-024-02448-8.
Outpatient care is central to both primary and tertiary levels in a health system. However, evidence is limited on outpatient differences between these levels, especially in South Asia. This study aimed to describe and compare the morbidity profile (presenting morbidities, comorbidities, multimorbidity) and pharmaceutical management (patterns, indicators) of adult outpatients between a primary and tertiary care outpatient department (OPD) in Sri Lanka.
A comparative study was conducted by recruiting 737 adult outpatients visiting a primary care and a tertiary care facility in the Kandy district. A self-administered questionnaire and a data sheet were used to collect outpatient and prescription data. Following standard categorisations, Chi-square tests and Mann‒Whitney U tests were employed for comparisons.
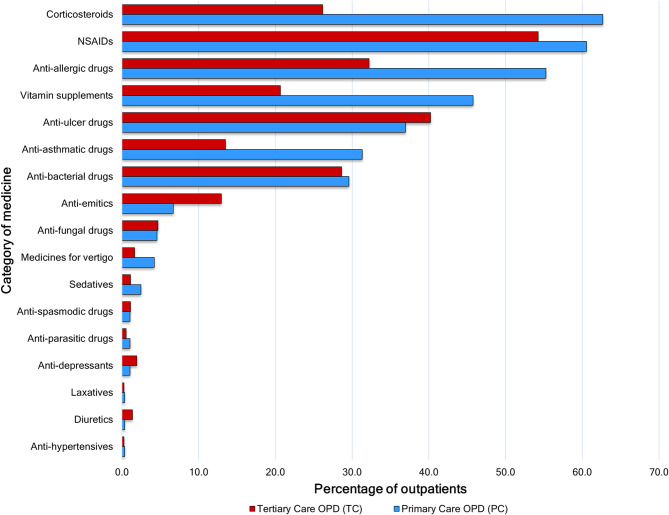
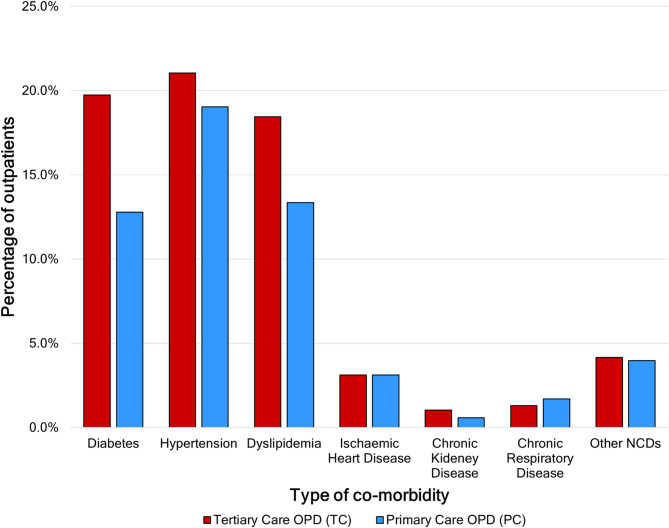
Outpatient cohorts were predominated by females and middle-aged individuals. The median duration of presenting symptoms was higher in tertiary care OPD (10 days, interquartile range: 57) than in primary care (3 days, interquartile range: 12). The most common systemic complaint in primary care OPD was respiratory symptoms (32.4%), whereas it was dermatological symptoms (30.2%) in tertiary care. The self-reported prevalence of noncommunicable diseases (NCDs) was 37.9% (95% CI: 33.2-42.8) in tertiary care OPD and 33.2% (95% CI: 28.5-38.3) in primary care; individual disease differences were significant only for diabetes (19.7% vs. 12.8%). The multimorbidity in tertiary care OPD was 19.0% (95% CI: 15.3-23.1), while it was 15.9% (95% CI: 12.4-20.0) in primary care. Medicines per encounter at primary care OPD (3.86, 95% CI: 3.73-3.99) was higher than that at tertiary care (3.47, 95% CI: 3.31-3.63). Medicines per encounter were highest for constitutional and respiratory symptoms in both settings. Overall prescribing of corticosteroids (62.7%), vitamin supplements (45.8%), anti-allergic (55.3%) and anti-asthmatic (31.3%) drugs was higher in the primary care OPD, and the two former drugs did not match the morbidity profile. The proportion of antibiotics prescribed did not differ significantly between OPDs. Subgroup analyses of drug categories by morbidity largely followed these overall differences.
The morbidities between primary and tertiary care OPDs differed in duration and type but not in terms of multimorbidity or most comorbidities. Pharmaceutical management also varied in terms of medicines per encounter and prescribed categories. This evidence supports planning in healthcare and provides directions for future research in primary care.
门诊服务是医疗体系中初级保健和三级保健的核心内容。然而,有关这两个层次之间门诊差异的证据有限,特别是在南亚。本研究旨在描述和比较斯里兰卡初级保健和三级保健门诊部门(OPD)成年门诊患者的发病情况(现有疾病、合并症、多种疾病)和药物管理(模式、指标)。
通过在康提地区招募 737 名成年门诊患者,进行了一项比较研究。使用自我管理问卷和数据表收集门诊和处方数据。采用标准分类后,采用卡方检验和曼-惠特尼 U 检验进行比较。
门诊患者队列以女性和中年人群为主。在三级保健 OPD 中,现有症状的中位数持续时间较长(10 天,四分位距:57),而在初级保健中为 3 天(四分位距:12)。初级保健 OPD 中最常见的全身症状是呼吸道症状(32.4%),而三级保健中则是皮肤病症状(30.2%)。自我报告的非传染性疾病(NCDs)患病率在三级保健 OPD 中为 37.9%(95%CI:33.2-42.8),在初级保健中为 33.2%(95%CI:28.5-38.3);仅糖尿病的个体疾病差异显著(19.7% vs. 12.8%)。三级保健 OPD 的多病共存为 19.0%(95%CI:15.3-23.1),而初级保健 OPD 为 15.9%(95%CI:12.4-20.0)。初级保健 OPD 的每次就诊药物数量(3.86,95%CI:3.73-3.99)高于三级保健 OPD(3.47,95%CI:3.31-3.63)。在两种情况下,每次就诊药物数量最高的都是用于治疗全身症状和呼吸道症状的药物。皮质类固醇(62.7%)、维生素补充剂(45.8%)、抗变态反应药(55.3%)和抗哮喘药(31.3%)的总体处方率在初级保健 OPD 中更高,且前两种药物与发病情况不匹配。OPD 之间抗生素的处方比例无显著差异。根据发病情况对药物类别进行的亚组分析在很大程度上遵循了这些总体差异。
初级保健和三级保健 OPD 之间的发病情况在持续时间和类型上存在差异,但在多发病或大多数合并症方面没有差异。药物管理在每次就诊药物数量和开方类别方面也存在差异。这一证据支持医疗保健规划,并为初级保健的未来研究提供了方向。