Khoury Shafik, Zornitzki Lior, Laufer-Perl Michal, Bhatia Raghav T, Marwaha Sarandeep, Tome Maite, Granot Yoav, Gvili Perelman Moran, Avivi Ido, Shacham Yacov, Szekely Yishay, Banai Shmuel, Hochstadt Aviram, Flint Nir, Topilsky Yan
Department of Cardiology, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel.
Tel Aviv University, Tel Aviv, Israel.
Int J Cardiol Heart Vasc. 2024 May 27;53:101427. doi: 10.1016/j.ijcha.2024.101427. eCollection 2024 Aug.
In many conditions characterised by septal hypertrophy, females have been shown to have worse outcomes compared to males. In clinical practice and research, similar cutoff points for septal hypertrophy are still used for both sexes. Here, we explore the association between different cutoff points for septal hypertrophy and survival in relation to sex.
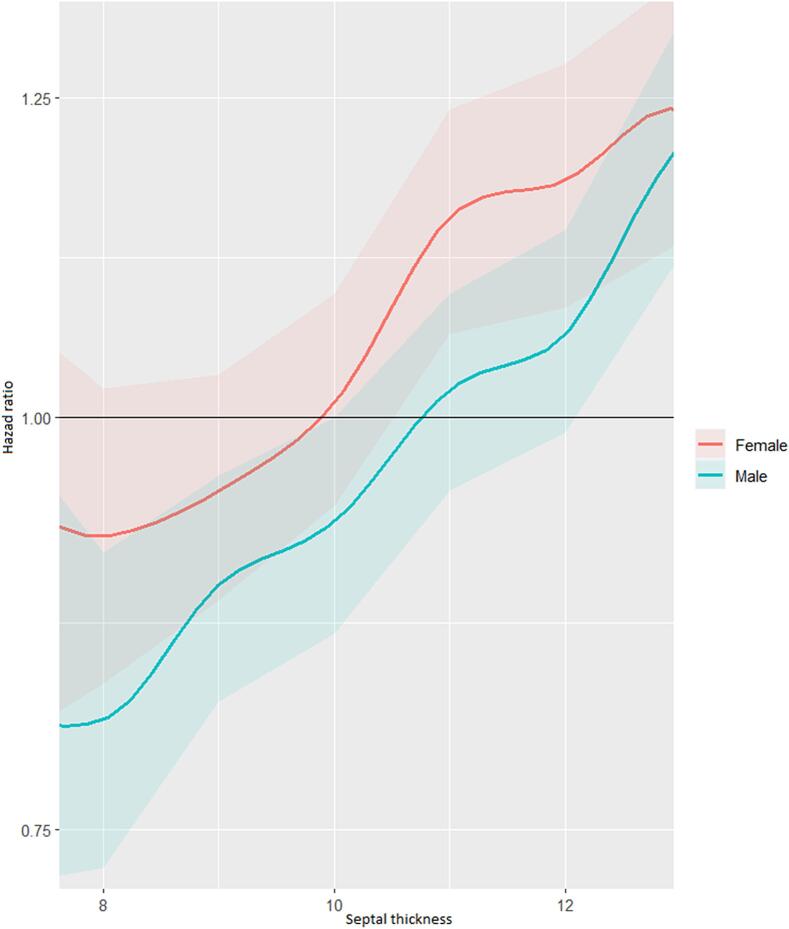
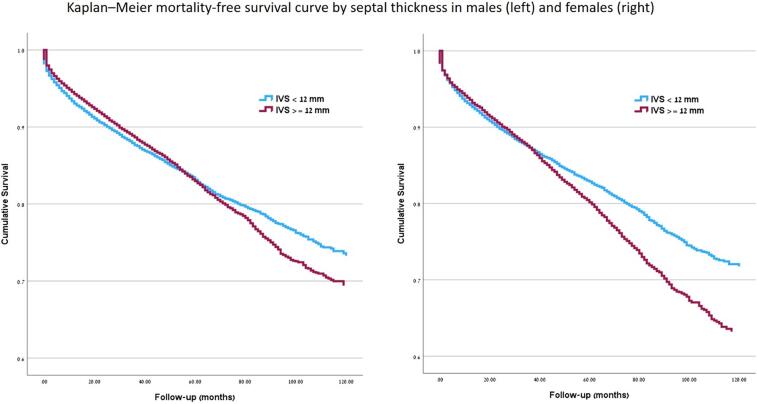
We performed a retrospective analysis of consecutive patients undergoing echocardiography between March 2010 and February 2021 in a large tertiary referral centre. A total of 70,965 individuals were included. Over a mean follow-up period of 59.1 ± 37 months, 9631 (25 %) males and 8429 (26 %) females died. When the same cutoff point for septal hypertrophy was used for both sexes, females had worse prognosis than males. The impact of septal hypotrophy on survival became statistically significant at a lower threshold in females compared to males: 11.1 mm (HR 1.13, CI 95 %:1.03-1.23, p = 0.01) vs 13.1 mm (HR 1.21, CI 95 %: 1.12-1.32, p < 0.001). However, when indexed wall thickness was used, the cutoff points were 6 mm/body surface area (BSA) (HR 1.08, CI 95 %: 1-1.18, p = 0.04) and 6.2 mm/BSA (HR 1.07, CI 95 %: 1-1.15, p = 0.05) for females and males, respectively.
Septal hypertrophy is associated with increased mortality at a lower threshold in females than in males. This may account for the worse prognosis reported in females in many conditions characterised by septal hypertrophy. Applying a lower absolute value or using indexed measurements may facilitate early diagnosis and improve prognostication in females.
在许多以室间隔肥厚为特征的疾病中,女性的预后相较于男性更差。在临床实践和研究中,室间隔肥厚的相似临界值仍用于两性。在此,我们探讨室间隔肥厚的不同临界值与生存之间的关联以及性别差异。
我们对2010年3月至2021年2月期间在一家大型三级转诊中心接受超声心动图检查的连续患者进行了回顾性分析。共纳入70965例个体。在平均59.1±37个月的随访期内,9631例(25%)男性和8429例(26%)女性死亡。当两性使用相同的室间隔肥厚临界值时,女性的预后比男性更差。与男性相比,室间隔变薄对女性生存的影响在更低阈值时具有统计学意义:11.1毫米(HR 1.13,95%CI:1.03 - 1.23,p = 0.01)对比13.1毫米(HR 1.21,95%CI:1.12 - 1.32,p < 0.001)。然而,当使用指数化壁厚度时,女性和男性的临界值分别为6毫米/体表面积(BSA)(HR 1.08,95%CI:1 - 1.18,p = 0.04)和6.2毫米/BSA(HR 1.07,95%CI:1 - 1.15,p = 0.05)。
室间隔肥厚与女性低于男性的更低阈值下的死亡率增加相关。这可能解释了在许多以室间隔肥厚为特征的疾病中女性报告的较差预后。应用更低的绝对值或使用指数化测量可能有助于女性的早期诊断并改善预后。