Hurkat Aditya, Sundaram Gidean A, Krishna Vinod K, Krishnan Murugesan, Kumar Santhosh P
Oral and Maxillofacial Surgery, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, IND.
Cureus. 2024 May 6;16(5):e59763. doi: 10.7759/cureus.59763. eCollection 2024 May.
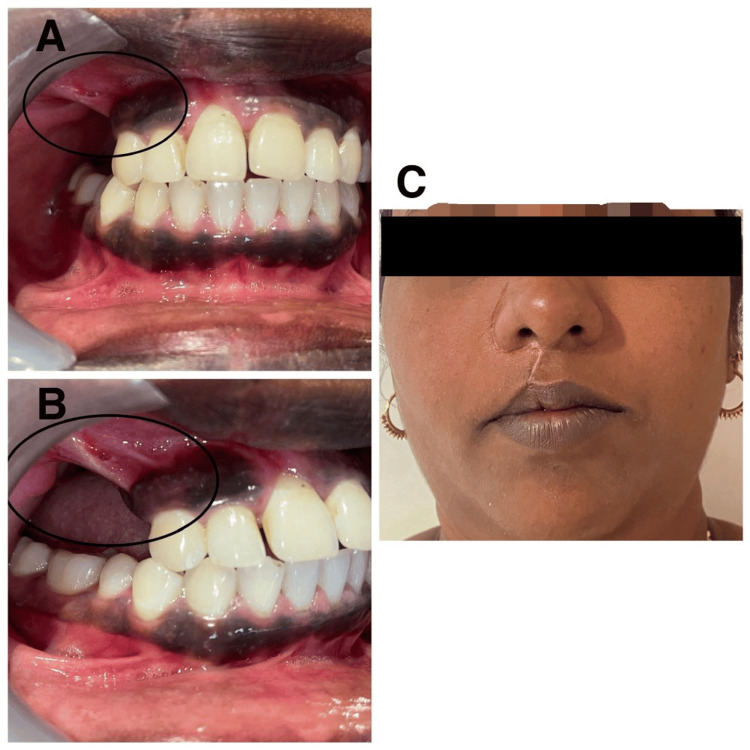
Odontogenic fibromyxoma typically presents as painless swelling in the jaw, and clinically, it grows slowly, becoming benign and asymptomatic. It causes the cortical plates to expand gradually, which leads to mobility and drifting of the teeth. Root resorption is also common. The tumor is locally aggressive in nature. It is also known to have a high recurrence rate. We present the case of a 30-year-old female patient who was diagnosed and treated for odontogenic fibromyxoma of the maxilla conservatively with enucleation. The radiograph showed a multilocular lesion, which can be confused with ameloblastoma, aneurysmal bone cyst, or odontogenic keratocyst. Hence, with proper clinical, radiographic, and histopathological examination, a correct diagnosis can be made and adequate treatment can be planned.
牙源性纤维黏液瘤通常表现为颌骨无痛性肿胀,临床上生长缓慢,呈良性且无症状。它导致皮质骨板逐渐扩张,进而引起牙齿松动和移位。牙根吸收也很常见。该肿瘤本质上具有局部侵袭性,且已知复发率高。我们报告一例30岁女性患者,她被诊断为上颌骨牙源性纤维黏液瘤,并通过摘除术进行了保守治疗。X线片显示为多房性病变,可能与成釉细胞瘤、动脉瘤样骨囊肿或牙源性角化囊肿相混淆。因此,通过适当的临床、影像学和组织病理学检查,可以做出正确诊断并制定适当的治疗方案。