Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
China National Clinical Research Center for Neurological Diseases, Beijing, China.
Cancer Med. 2024 Jun;13(11):e7377. doi: 10.1002/cam4.7377.
The study aimed to identify if clinical features and survival outcomes of insular glioma patients are associated with our classification based on the tumor spread.
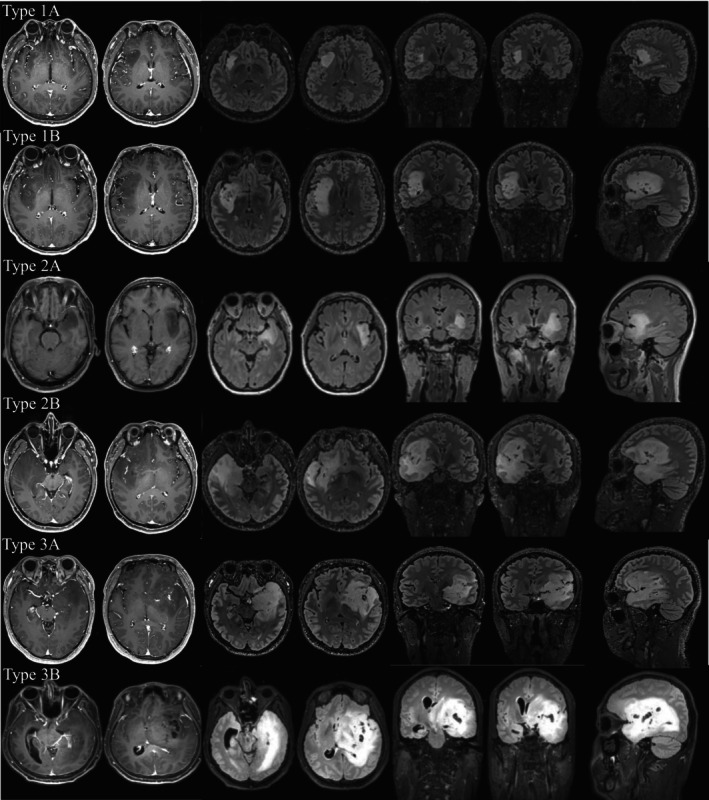
Our study included 283 consecutive patients diagnosed with histological grade 2 and 3 insular gliomas. A new classification was proposed, and tumors restricted to the paralimbic system were defined as type 1. When tumors invaded the limbic system (referred to as the hippocampus and its surrounding structures in this study) simultaneously, they were defined as type 2. Tumors with additional internal capsule involvement were defined as type 3.
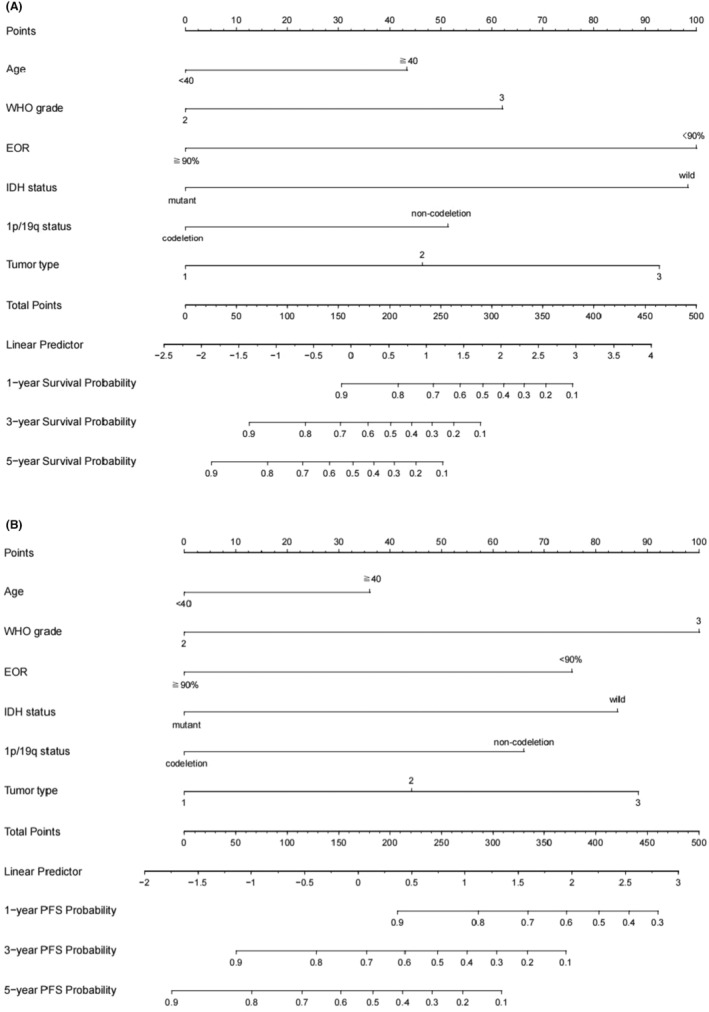
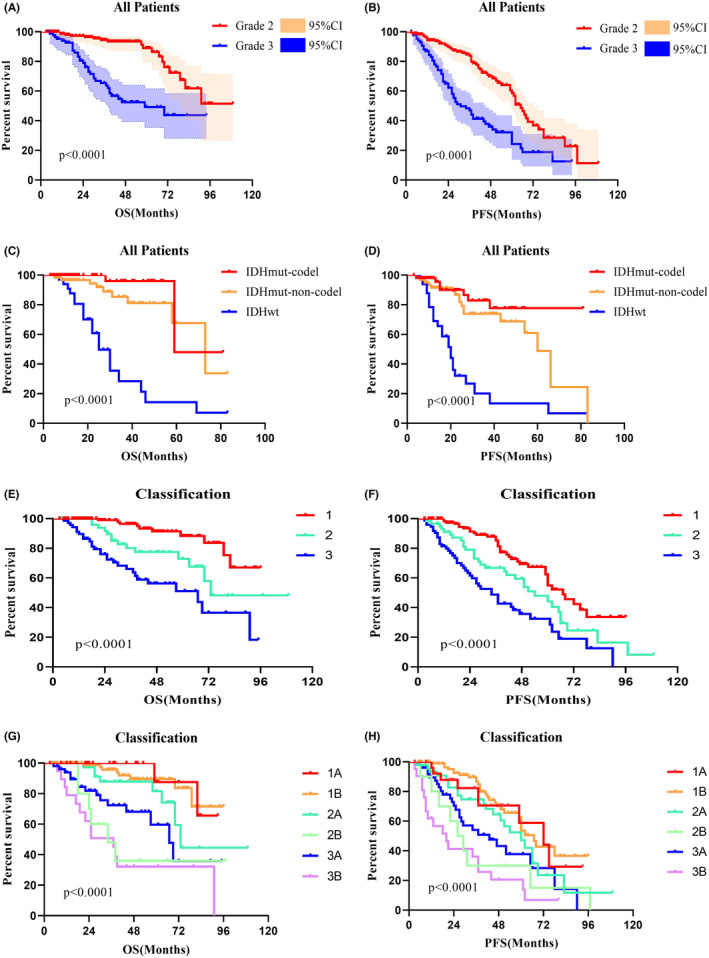
Tumors defined as type 3 had a higher age at diagnosis (p = 0.002) and a higher preoperative volume (p < 0.001). Furthermore, type 3 was more likely to be diagnosed as IDH wild type (p < 0.001), with a higher rate of Ki-67 index (p = 0.015) and a lower rate of gross total resection (p < 0.001). Type 1 had a slower tumor growth rate than type 2 (mean 3.3%/month vs. 19.8%/month; p < 0.001). Multivariate Cox regression analysis revealed the extent of resection (HR 0.259, p = 0.004), IDH status (HR 3.694, p = 0.012), and tumor spread type (HR = 1.874, p = 0.012) as independent predictors of overall survival (OS). Tumor grade (HR 2.609, p = 0.008), the extent of resection (HR 0.488, p = 0.038), IDH status (HR 2.225, p = 0.025), and tumor spread type (HR 1.531, p = 0.038) were significant in predicting progression-free survival (PFS).
The current study proposes a classification of the insular glioma according to the tumor spread. It indicates that the tumors defined as type 1 have a relatively better nature and biological characteristics, and those defined as type 3 can be more aggressive and refractory. Besides its predictive value for prognosis, the classification has potential value in formulating surgical strategies for patients with insular gliomas.
本研究旨在确定岛叶胶质瘤患者的临床特征和生存结局是否与我们基于肿瘤扩散的分类有关。
我们的研究纳入了 283 例组织学 2 级和 3 级岛叶胶质瘤患者。提出了一种新的分类方法,将仅限于边缘系统的肿瘤定义为 1 型。当肿瘤同时侵犯边缘系统(在本研究中指海马及其周围结构)时,定义为 2 型。肿瘤伴有额外的内囊受累,定义为 3 型。
诊断为 3 型的肿瘤患者诊断时年龄较大(p=0.002),术前体积较大(p<0.001)。此外,3 型更可能被诊断为 IDH 野生型(p<0.001),Ki-67 指数较高(p=0.015),大体全切除率较低(p<0.001)。1 型肿瘤的生长速度比 2 型慢(平均增长率为 3.3%/月 vs. 19.8%/月;p<0.001)。多变量 Cox 回归分析显示,切除范围(HR 0.259,p=0.004)、IDH 状态(HR 3.694,p=0.012)和肿瘤扩散类型(HR=1.874,p=0.012)是总生存(OS)的独立预测因素。肿瘤分级(HR 2.609,p=0.008)、切除范围(HR 0.488,p=0.038)、IDH 状态(HR 2.225,p=0.025)和肿瘤扩散类型(HR 1.531,p=0.038)对无进展生存(PFS)有显著影响。
本研究根据肿瘤扩散提出了一种岛叶胶质瘤分类方法。结果表明,定义为 1 型的肿瘤具有相对较好的性质和生物学特征,而定义为 3 型的肿瘤可能更具侵袭性和难治性。除了对预后有预测价值外,该分类方法对制定岛叶胶质瘤患者的手术策略具有潜在价值。