Idowu Jeuel O, Idowu Olufemi, Oyeleke Stephen O
Finnih Medical Centre, Ikeja, Lagos, Nigeria.
Division of Neurological Surgery, Department of Surgery, Faculty of Clinical Sciences, College of Medicine, Lagos State University, Ikeja, Lagos, Nigeria.
Niger Med J. 2022 Sep 12;63(4):312-320. doi: 10.60787/NMJ-63-4-75. eCollection 2022 Jul-Aug.
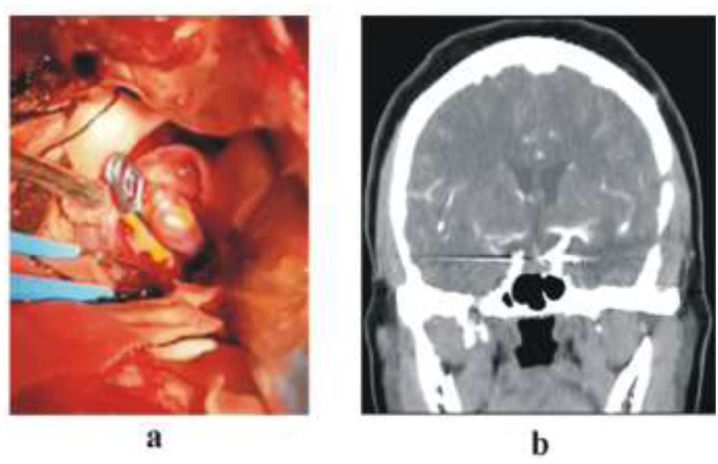
Ruptured cerebral artery aneurysms (RCAA) are devastating diseases with high morbidity and mortality rates if not promptly managed. In Nigeria, access to timely neurosurgical services remains a challenge and aneurysm coiling is still not possible in virtually all centres in Nigeria. The aim of this study is to report on our 9 years' experience with clipping of cerebral aneurysm and on the attendant clinical outcomes.
A retrospective analysis of all consecutive operated RCAA between March 2012 and June 2021 was conducted. Patients' demographic parameters, World Federation of Neurosurgical Societies (WFNS) grade, Hunt and Hess (HH) grade, aneurysm location, timing of surgery and outcome were analysed. Outcome was measured using Glasgow Outcome Scale (GOS) score.
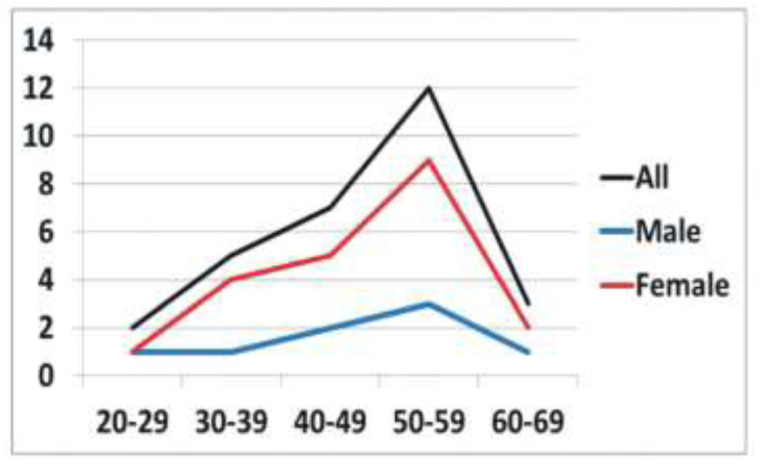
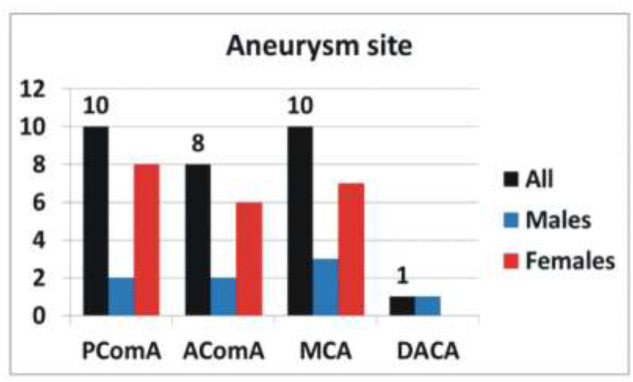
A total 29 were included in the study. The most common age group affected was between 50-59 years. RCAA were mainly in the region of the middle cerebral artery and posterior communicating artery (PComA) territories. All the patients presented after 24 hours of the ictus. Two (6.9%) patients had multiple aneurysms. Early clipping (<72hours after presentation) was possible in 8 (27.6%) patients. At least one episode of a rebleed occurred in 19 (65.5%) patients prior to surgery. Mortality rate was 17.2%. None of the patients with PComA aneurysm died. The patients' pre-operative WFNS and HH grades were significantly associated with GOS.
Modifiable factors like under diagnoses, delayed referral, cultural belief and financial challenges may account for the low number of patients presenting for neurosurgical care. The possibility of a sizeable number of patients dying due to these factors is a strong possibility for the low number of patients presenting for neurosurgical care.
破裂性脑动脉瘤(RCAA)是一种严重的疾病,如果不及时治疗,发病率和死亡率都很高。在尼日利亚,获得及时的神经外科服务仍然是一项挑战,而且在尼日利亚几乎所有中心都无法进行动脉瘤栓塞术。本研究的目的是报告我们9年来夹闭脑动脉瘤的经验及随之而来的临床结果。
对2012年3月至2021年6月期间所有连续接受手术的RCAA患者进行回顾性分析。分析患者的人口统计学参数、世界神经外科协会联合会(WFNS)分级、Hunt和Hess(HH)分级、动脉瘤位置、手术时机和结果。使用格拉斯哥预后量表(GOS)评分来衡量结果。
本研究共纳入29例患者。受影响最常见的年龄组为50 - 59岁。RCAA主要位于大脑中动脉区域和后交通动脉(PComA)区域。所有患者均在发病24小时后就诊。2例(6.9%)患者有多个动脉瘤。8例(27.6%)患者能够早期夹闭(就诊后<72小时)。19例(65.5%)患者在手术前至少发生过一次再出血。死亡率为17.2%。PComA动脉瘤患者无一死亡。患者术前的WFNS和HH分级与GOS显著相关。
可改变的因素,如诊断不足、转诊延迟、文化信仰和经济挑战,可能是接受神经外科治疗的患者数量较少的原因。由于这些因素,相当数量的患者可能死亡,这很可能是接受神经外科治疗的患者数量较少的原因。